Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
25 Cultural Highlight Section 2 – Explore Mexican-American Culture
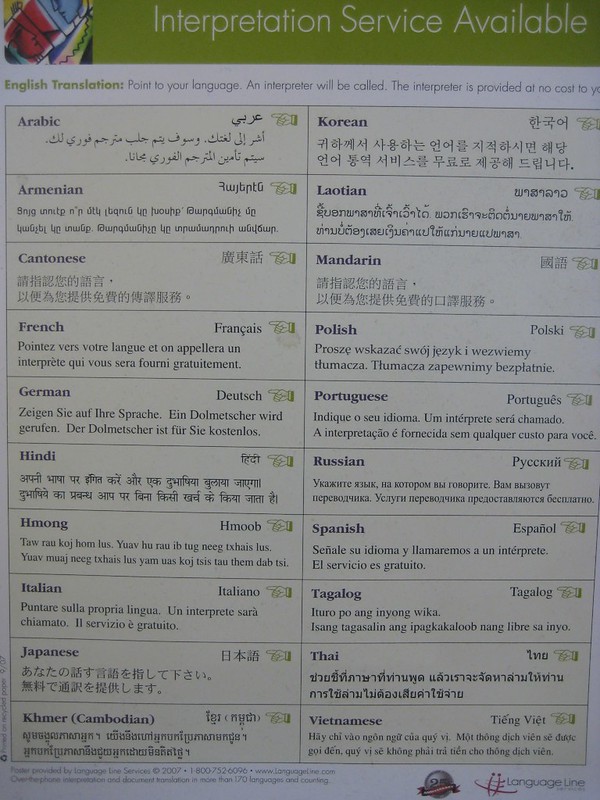
Cultural Highlight: Mexican-American Culture
“Nearly 4 in 10 Mexican Minnesotans live outside of the Twin Cities. 38% of Mexican Minnesotans live in greater Minnesota” (Cultural Compass, 2021).
Anahy shares her culture.
Section One Learning Outcomes
After reading and considering this Unit, students will:
Learn basic facts about Mexican and Mexican-American cultures, primarily those living in and with cultural and social ties to Minnesota
Understand identity and distinguish between personal, social, and cultural identities, respectively
Identify some of the barriers that lead to identity disconfirmation: stereotypes, implicit and explicit bias, prejudice, and discrimination
Practice paraphrasing and perception checks
Visting E.L. Burrito in St. Paul Photo: Lori HW
Introduction:
When seeking to understand the “culture(s) in your backyard” in Minnesota, with Mexican culture, one should not overgeneralize as to who is “American” and be quick to label or stereotype who is undocumented. This section will consider Maro’s story to understand the importance of constructed and complex personal, social, and cultural identities. We will turn towards how, during the communication process,stereotypes, implicit and explicit bias, and prejudice derail opportunities to create genuine, compassionate intercultural communication. Indeed, stereotypes, biases, and prejudice prevent the development of communication competencies that help overcome the notion of treating those of an unknown and foreign culture as an “Other“–an object of suspicion and fear. Communication strategies that build intercultural communication competency are found in the Cultural Atlas on Mexican communication styles and some “do’s and don’ts” of Mexican culture. We will highlight Minnesota historical stories, timelines, and special topics as other units. This unit pulls together a wide variety of materials you have already learned with the goal of sharing how the theories related to Intercultural Communication can be applied to learn about a particular culture or co-culture.
Additionally, in this Chapter, we will also share stories of past students including Marco and Fredy. Fredy’s interview was conducted with RCTC’s Dental Hygiene instructor Katie Ristau and Spanish Instructor, Lillyam Arroyave (Lillyam.Arroyave@rctc.edu). We have combined Fredy’s interview with materials previously published on intercultural communication and Medical Care.
Due to Mexico’s proximity to the United States, Mexican-Americans perhaps experience a connection to their country of origin on a more immediate level than other immigrant groups from countries much further away. Mexican-Americans have shared many different immigration stories. Some families immigrated numerous generations ago, while others are still arriving today. Indeed, some individuals who identify as Mexican-American have roots in families who lived in Texas long before it was colonized. No one story epitomizes Mexican immigration. The Minnesota Historical Society has curated and preserved some timelines that can help better understand how Mexicans settled in Minnesota, depending upon their own cultural and institutional supports–e.g., grocery stores, churches, and restaurants.
Marco expands upon the many concerns and worries that Mexican-Americans and Mexican nationals living in the United States face in his interview. Type into one’s browser “Mexican border,” and you will find daily news stories about the U.S./Mexican border. Now scroll down and note the comments; what do you notice? In conversation with Marco, he shared that being called or named “illegal” (v.s. “undocumented“) elicits a crushing, degrading feeling. Again, language has the power to define cultures, societies, groups, and individuals. Look back to the chapter on verbal communication and consider the powerful self-defining and perception-shaping quality language possesses. Marco works as a community organizer, understands, and erases the degradation caused by the ignorant or malicious use of language.
Who am I, who are you, what are we doing here together? Photo by Lori HW
Personal, Social, and Cultural Identities
*Attribution: materials in this subsection are built upon Grothe’s (2021) OER book.
The phrase “who am I, who are you, and what are we doing here together,” mentioned at this book’s beginning and subsequently, is a means of approaching, examining, and thinking through the communication process. It is a way to view the complexity of the communication process, the formation of identity within and through that process, and the hope for competent and compassionate intercultural communication.
Perhaps the fundamental function of identity is to give meaning through self-definition. Remember, identity is complex, fluid, abstract, dynamic, and socially constructed. Thus, identity is not a static, singular entity. Instead, identity is dynamic and contextual, formed through interaction or intersection with others (from a different culture, society, or group) and through the individual’s intrapersonal processing of interpersonal, group, and institutional communication and messaging. Focus is placed on three aspects of identity and their interplay that work to shape our self-concept: personal, social, and cultural.
In this vein, Grothe posits:
Ask yourself the question “Who am I?” Recall from our earlier discussion of self-concept that we develop a sense of who we are based on what is reflected back on us from other people. Our parents, friends, teachers, and the media help shape our identities. While this happens from birth, most people in Western societies reach a stage in adolescence where maturing cognitive abilities and increased social awareness lead them to begin to reflect on who they are. This begins a lifelong process of thinking about who we are now, who we were before, and who we will become (Tatum, B. D., 2000).
…Any of these identity types can be ascribed or avowed. Ascribed identities are personal, social, or cultural identities that are placed on us by others, while avowed identities are those that we claim for ourselves (Martin & Nakayama, 2010). Sometimes people ascribe an identity to someone else based on stereotypes (Grothe, 2021).
To better understand these concepts, it helps to use an extended example to show the distinctions. Marco shared many details about his lived experiences in the video above and demonstrated the materials from the OER text Grothe (2021) authored.
Personal Identities
photo: Amy Tran – unsplash.com
Grothe (2021) reminds us that, “We must avoid the temptation to think of our identities as constant. Instead, our identities are formed through processes that started before we were born and will continue after we are gone; therefore our identities aren’t something we achieve or complete. Two related but distinct components of our identities are our personal and social identities (Spreckels, J. & Kotthoff, H., 2009). Personal identities include the components of self that are primarily intrapersonal and connected to our life experiences” (Grothe, 2021).
Marco’s love for travel, music, family, and finding great local restaurants becomes apparent. He has shared a passion for helping others and his mother’s cooking in conversations. He also implies his self-concept when he states, “I want to be a person who my parents could have turned to when they first arrived.” These passions for life have driven and shaped Marco’s identities: Mexican living in the United States, traveler, soccer enthusiast, lover of food, mama’s boy (he agrees), and helper. In the video, he often refers to himself as “undocumented.” This status, too, becomes a personal identity. As a reminder, though, Marco may have many likes that are not necessarily unique or related to his DACA status or Mexican citizenship. He enjoys reading, singing, and dancing. As one can see, though, the experiences he had in the United States compared to his experiences in Mexico offered him different choices to build a set of experiences where he could discover his: “I like ___ and I do not like ____.”
Marco shares how he thought he would return to Mexico anytime and clarifies that he did not desire to engage in school activities. His avowed personal identity became: “non-participant” and “non-academic.” He shares how a persistent and compassionate high school teacher did not give up on him. One of Marco’s teachers told him that “you are a good student, and you will be staying here for your education.” His teacher’s comment is an example of a positive ascribed personal identity. Marco shares how his teacher’s remark changed his life and educational path. This example illustrates the essential nature communication–even if brief–plays in building one’s personal identity. Sadly, not all students receive this intervening message.
Traditional children’s toys Photo: Lori HW
Sample Reflection Activity
List 5 messages you remember hearing in school about who you were. These could be These messages could be from peers, older/younger students, teachers, staff, etc.
How did these messages impact your educational trajectory?
Describe one avowed personal identity you hold/did hold as a student.
Describe one ascribed personal identity you hold/did hold as a student.
Social Identities
Our social identities are the components of the self, created from involvement in social groups to which we are interpersonally committed. For example, we may derive aspects of our social identity from our family or a community of fans for a sports team. Social identities differ from personal identities because they are externally organized through membership. Our membership may be voluntary (Maro is a member and leader in the group UNICOS MN) or involuntary (family), explicit (Marco pays a fee to continue to be a DACA member), or implicit (we purchase and listen to our favorite music genre). There are numerous options for personal and social identities. While our personal identity choices express who we are, our social identities align with particular groups. Samavor (2017) reminds us, “as situations vary, you usually choose to emphasize one or more of your identities” (p. 247). In ninth grade, Marco shares that he did not try. Consider Marco’s detailed description of this time in his life:
Marcos explains his story.
I grew up very insecure about whether I was going back to Mexico or not. And I decided not to try hard in school I decided, ‘what’s the point, if I’m going to be brought to Mexico with my parents because this was always on the table. There was always the knowledge of,’We are here to work, build our house…so we can go back and you will start school there. And you will make your life over there.’ So at that point I struggled a lot and I have to be very thankful to an advisor at Mayo High School, his name was Mr. Mulugeta Haileab. He passed away recently. He may he maybe doesn’t know the effects that he had on me. But it was like life-changing way because I I it was ninth grade and I knew that I was gonna go back to Mexico. I was just in my head. There’s no way that I’m going to stay back and I’m not sure if he just knew or what it was. But he said Just keep trying. He’s like You’re going back. It’s like trust me, you’re not going back….You know, I’m still here. I finished high school.
Mr. Mulugeta Haileab, in Marco’s life, told him that today was important and that today he was a Mayo High School student in Rochester, MN. Mr. Haileab gave Marco explicit messages affirming Marco’s social identity as a student in the United States. These are all examples of “ascribed” social identities. Marco begins to accept the social identity, transforming it into an “avowed” social identity. When he changes his mindset and behavior, he can see changes in his grades.
As a consequence, he can reshape his personal identity. At the same time, though, he is receiving competing and conflicting ascribed social identity messages: you are here with us as your family, we will go back to Mexico where you will start your job vs. you are a good student and I, as a teacher, will not give up on you. In contrast, some media and even some of his fellow Mayo High School classmates tell him, “you are illegal, go back to where you belong.”
photo: pexel.com
Through our social identities, we make statements about who we are and who we are not.” Marco’s video examples of “social identities” include a past Mayo High School student, a Rochester resident, not American, a part of his family who only came to work here and return. Some social identities that are “ascribed” by others and “placed upon him” could include: “illegals.” Marco mentions that becoming a DACA recipient also changed his life. Group membership is a form of social identity. Once he became a DACA recipient, his legal status was also restored, allowing him also to enhance his personal identity, “I am a DACA and became a Driver. I can fly. I can get my degree but not practice it.” Now, he can experience more of the activities other young people have experienced. HIs restored legal status allows Marco to develop new interests and hobbies and helps him expand his personal identity. At the same time, he has this competition with his social identity, “I am just dreaming.” He shares that sometimes the “dream becomes a nightmare.”
photo: pexel.com
Sample Reflection Activity
List 5 social groups you belong to. Next to the social group, name an “avowed social identity” and an “ascribed social identity” aligned with that social group membership.
Sample: I am enrolled at RCTC: one avowed social identity I hold is that of a frugal college student, one ascribed identity I feel is “JUST a 2-year student.”
Cultural Identities
Another area of identity includes messages from our culture. To review, Communication in the Real World (2016) asserts:
Culture is a complicated word to define, as there are at least six common ways that culture is used in the United States. For the purposes of exploring the communicative aspects of culture, we will define culture as the ongoing negotiation of learned and patterned beliefs, attitudes, values, and behaviors. Unpacking the definition, we can see that culture shouldn’t be conceptualized as stable and unchanging. Culture is ‘negotiated,’ and as we will learn later in this chapter, culture is dynamic, and cultural changes can be traced and analyzed to better understand why our society is the way it is. The definition also points out that culture is learned, which accounts for the importance of socializing institutions like family, school, peers, and the media. Culture is patterned in that there are recognizable widespread similarities among people within a cultural group. There is also deviation from and resistance to those patterns by individuals and subgroups within a culture, which is why cultural patterns change over time. Last, the definition acknowledges that culture influences our beliefs about what is true and false, our attitudes including our likes and dislikes, our values regarding what is right and wrong, and our behaviors. It is from these cultural influences that our identities are formed.
Concerning cultural identities, Grothe further explains:
Members of Indigenous Roots share their talents and prayers at Indiginious Persons Day, 2021 | photo, Lori HW
Cultural identities are based on socially constructed categories that teach us a way of being and include expectations for social behavior or ways of acting (Yep, G. A., 2002). Since we are often a part of them since birth, cultural identities are the least changeable of the three. The ways of being and the social expectations for behavior within cultural identities do change over time, but what separates them from most social identities is their historical roots (Collier, M. J., 1996). Additionally, common ways of being and acting within a cultural identity group are expressed through communication. In order to be accepted as a member of a cultural group, members must be acculturated, essentially learning and using a code that other group members will be able to recognize. We are acculturated into our various cultural identities in obvious and less obvious ways. We may literally have a parent or friend tell us what it means to be a man or a woman. We may also unconsciously consume messages from popular culture that offers representations of gender (Grothe, 2021).
Marco mentions he was not considered to be fully American by a lot of people here. But even if I would go back to my country, I wouldn’t be considered a Mexican either.” He later shares that many people fall between cultural identities as part of DACA. “The power of ascribed cultural identities includes when they are perpetuating a stereotype” (Grothe, 2021). President Donald Trump stated, “When do we beat Mexico at the border? They’re laughing at us, at our stupidity,” Trump said as he announced his candidacy on June 16, 2015. “And now they are beating us economically. They are not our friends, believe me. But they’re killing us economically. The U.S. has become a dumping ground for everybody else’s problems” (Reilly, 2016). Many people agree with President Trump, and we recognize you might as well. Regardless of our cultural identity, we all fall victim to ethnocentric thinking. Grothe (2021) explains,
Such attitudes are an example of ethnocentrism, placing one’s own culture and the corresponding beliefs, values, and behavior categorizations of people based on their group affiliation. We stereotype people because it streamlines the perception process. Once we’ve categorized a person as a member of a particular group, we can form a quick impression of them (Macrae, et al., 1999). When we stereotype others, we replace human complexities of personality with broad assumptions about character and worth based on social group affiliation. We stereotype people in the perception process to help us make sense out of our world, which might be efficient for communication, but frequently leads us to form flawed impressions.
When we hold a stereotype about a person, we have expectations that he or she will fulfill that stereotype. A [pb_glossary id="1671"]self-fulfilling prophecy is an expectation held by a person that alters his or her behavior in a way that tends to make it true. When we hold stereotypes about a person, we tend to treat the person according to our expectations. This treatment can influence the person to act according to our stereotypic expectations, thus confirming our stereotypic beliefs.
Self-fulfilling prophecies are ubiquitous—even teachers’ expectations about their students’ academic abilities can influence the students’ school performance (Jussim, Robustelli, & Cain, 2009).
In Marco’s story, we hear how impacting his Mayo High School advisor’s words were. Marco mentions that he doesn’t even think that Mr. Mulugeta Haileab knew the impact of his words. While Marco shares a positive effect, research by Rosenthal and Jacobson (1968) found that disadvantaged students whose teachers expected them to perform well had higher grades than disadvantaged students whose teachers expected them to do poorly.
photo: pexel.com
Confirmation Bias
Finally, we’ll consider the power of confirmation bias. Fyock & Stangor(1994) shared that:
Stereotypes are maintained because information that confirms our stereotypes is better remembered than information that disconfirms them. In this process, known as confirmation bias, we seek out, conciously or unconciously, information that supports our stereotypes and ignores information that is inconsistent with our stereotypes (Grothe, 2021).
If we believe that individuals of Mexican descent living in the U.S. are “illegal,” and when we see someone on the news being deported due to being undocumented, then we tend to remember it. Still, when we see a person from the same cultural identity who graduates top of her class or somehow models mainstream social standards, we tend to forget it.
When we confirm our biases, we tend to perceive the world in ways that make it fit our existing beliefs, rather than changing our beliefs to fit the reality around us. Because they are so highly cognitively accessible, and because they seem so “right,” our stereotypes easily influence our judgments of and responses to those we have categorized (Grothe, 2021).
photo: pexel.com
Sample Reflection Activity
Consider Maro’s situation:
Maro shares he was born in 1994, and his parents migrated for the first time in 1999 when he was four years old. After two years, his brothers were in Mexico, so they returned to be with them. They spent three years in Mexico; they decided to come back to the United States.
In the first experience, they came to the U.S. undocumented. They crossed the border using the legal protocol with a visa on the second journey.
They knew they couldn’t go back and did become undocumented when they knowingly overstayed their travel visa.
Maro shares his fear and trauma from the first time he came, how they got separated. He talks about how he felt “just like other kids.” Then he learned, “I am not American.” He shared that he thought, If I went back to my own country, I would not be seen as an authentic Mexican.
Many messages went through his head: I am not a high driver; I am undocumented; I am not a gang-banger but might be perceived as such due to where we live.
The message, “you are going back to Mexico,” stayed with Marco. He began to “not try” in school. He began to fail. In 9th grade, his actions matched his personal expectations. His Mayo High School Advisor made a difference when Marco was in ninth grade.
Explain how Marco’s story is related to the self-fulfilling prophecy.
More on Implicit Bias
Consider the power of Implicit Bias – the Standford Encyclopedia Shares:
Research on “implicit bias” suggests that people can act on the basis of prejudice and stereotypes without intending to do so. While psychologists in the field of “implicit social cognition” study consumer products, self-esteem, food, alcohol, political values, and more, the most striking and well-known research has focused on implicit biases toward members of socially stigmatized groups, such as African-Americans, women, and the LGBTQ community.[1] For example, imagine Frank, who explicitly believes that women and men are equally suited for careers outside the home. Despite his explicitly egalitarian belief, Frank might nevertheless behave in any number of biased ways, from distrusting feedback from female co-workers to hiring equally qualified men over women. Part of the reason for Frank’s discriminatory behavior might be an implicit gender bias. Psychological research on implicit bias has grown steadily (§1), raising metaphysical (§2), epistemological (§3), and ethical questions (§4).[2]
Anahy took Lori on a tour of her favorite place in St. Paul. Listen to her impromptu speech (a sample for a Public Speaking assignment to introduce the class to a new site).
Suggested Activity!
It Tastes So Good! But what are we eating and why, I wouldn’t know the difference. Have you said this? In the following video, I find myself even saying that. I have always enjoyed cooking and, well – eating! I explore the world with food. Others in my family will ask for the same Pace Salsa and only Pace. Let’s not shake it up! What about you?
I tried your assignment: Culture in my Backyard at El Burrito in St. Paul, MN.
I was not just running in and out in 15 minutes. I stayed 3 – THREE – hours with a trusted host. I learned so much. I know you might not take that much time nor find someone to give you such detailed information. I promise you, if you can push yourself to learn more, you can learn to make more complex perceptions. My goal in sharing the following information in this segment is to demonstrate how much I gained from such a short time.
“This how much we care for the flavors and our food, and that is what makes us different!” I was gifted with the time my student spent with me on a busy fall semester Saturday before her finals. We took several hours walking through her favorite Mexican Store in Saint Paul, Minnesota. I asked questions. SO MANY QUESTIONS. Do you worry you will ask the wrong question? I know that is a concern so many of my students’ voices, and, without exception, each semester, our class talks about how so many of us don’t ask so we won’t offend.
The Human Library offers an opportunity to ask ALL QUESTIONS. This is one suggestion, as an instructor, I highly suggest. I also have gained permission and welcome from several folks in Minnesota to personally ask questions for you (ok, and me) to learn more. Several folks featured in our video also welcome you to reach out to ask more. I can connect with you should you like to do so. Many of the individuals in our OER book will also offer conversation hours online or in person. Just ask.
In the following video, I decided not to edit our conversation. At this point, we had made about 5 videos already. We were laughing as we explored the whole store. I wish for you this same opportunity as I know it was a true gift she gave me. I love to travel and do the same thing (once asking a group of Scottish women in a small town we accidentally traveled to vs. our planned destination, what I should buy to make an “authentic Scottish meal.” It was as if our little Dodge Center Sunshine foods grocery store staff and customers all came to talk about which lefse to buy!). For your site visit, friends in Minnesota offer the same experience for you in Rochester or the Twin Cities.
In this video, note how many peppers there are. I say, “I wouldn’t know the difference.” This is an example of perception. She offers me new “categories” for my “sense-data” to “fit into.” This is expanding my organizational schemata. OK, big word.
My original perception – I see a dried packaged spice. I know it fits “hot chili pepper I can add to my Mexican cooking, it is HOT and SPICY, but I like it.
Selection = I see a dried packaged spice among SO MANY choices.
Organization = Hot pepper or Sweet pepper? I place it, due to my past experience, into “hot”
Interpretation = Therefore, I will buy it and like it in moderation as it fits my taste.
Oh, but there are degrees of HOT or sweet.
Anahy gives me over 5 choices for what I might have called,” a chili pepper.” in the past. This broadens my “organization schemata” in my perception. Just a bit more time on the internet, and I learned that there are more than 60 types of chiles with 13 “essential chile peppers” – 4 fresh and 9 dried chiles (and even a new spelling!). “With more than 60 types produced in Mexico, chiles are a fundamental component of Mexican cuisine. The wide array of chiles available in the country adds complexity, depth, and heat to countless dishes. Fresh chiles can be used to add color, texture, and heat to any dish” (MasterClass.com, 2020)
Selection = I see a dried packaged spice that is brown and larger than the red small pepper (notice how now I can SEE and SMELL different sense-data?)
Organization = I know 9 chiles now: Ancho, Cascabel, Guajiilo, Pasilla, Arbo, Mulato, Morita, Pulla, Pequin. (OK, so I might have a list and photos in front of me at first – or my smartphone to show me).
Interpretation = Therefore, I know this is Arbo I will personally buy it for my own salsa preparation.
In the past, I’d just use a “little” of the “chili pepper” as I want spice but not TOO MUCH! Did I know I could use different peppers for a different taste, well, yes (and my own children are now shaking their heads saying, yes, mom, we’ve told you, created this, and my own daughter in law, a talented agronomist grows many peppers with her friends. BUT, I didn’t know the nuances, I just used less or more, not different peppers. NOW I have choices! I know this based upon expanding my own experience in tasting, smelling, and learning about peppers.
MORAL: if I can learn this much about peppers, imagine how much there is out there to explore. Practice small changes. It can help you build confidence to try the next change!
Thank you Anahy Camposeco Rodriguez! I have learned so much and my leave-taking experience was so positive. This interaction helps me form a positive attachment to my experience.
Suggested Activity: Visit a local grocery store that is new to you. Our “Cultural in your Backyard Passport Hosts” know you are coming if you are in the Rochester, MN area. Let Lori know if you want someone to come with you or have one of the staff members greet you.
Explore Spices like an artist or a culinary student. You can try my “chile” sample above. How many did you find? Take some photos, take notes, buy a few if you can afford it.
Write: Describe at least 5 peppers with your 5 senses. Now, just like you did when you learned sentence structure, write out your perception for one of the peppers. If you are from or very familiar with the Mexican (or Hispanic) culture, you will obviously have even more keen observations, more complex organizational schemata, and perhaps a more refined interpretation. Nevertheless, just try it (or find a new culture to explore), to help map out your perception process. This will become a sample and perhaps a metaphor about how we can broaden our perceptions of not just food or as precise as the type of chile pepper we personally prefer for certain occasions, it is a means to unpack how we experience all of the world! Whew, a bit heady, right!?
Sample:
SELECTION – I notice this sense data:
Smell
Sight
Taste
Texture
Sound (? maybe when you break it in half?)
ORGANIZATION – I have these 5 chiles to compare that sense data to
Chile 1 is called ________________
Chile 2 is called ________________
Chile 3 is called ________________
Chile 4 is called ________________
Chile 5 is called ________________
INTERPRETATION – Due to my new knowledge, I can see that this is a______ pepper and I do/don’t like it for the particular dish I want to create.
Consider Language – From Communication in the Real World
The following is shared from the OER Textbook, Communication in the Real World. (2016). Note that the tern Latinix is not included.
Consider the September 23, 2021 Article, “Who is Hispanic? which questions:
“Debates over who is Hispanic and who is not have often fueled conversations about identity among Americans who trace their heritage to Latin America or Spain. Most recently, the 2020 census has drawn attention to some of the many layers of Hispanic identity, providing fresh details about how Hispanics view their racial identity. So, who is considered Hispanic in the United States? And how are they counted in public opinion surveys, voter exit polls and government surveys such as the 2020 census? The most common approach to answering these questions is straightforward: Who is Hispanic? Anyone who says they are. And nobody who says they aren’t”(Lopez,, Krogstad, & Passel, 2021).
Now, how would you update the following statement from the 2016 textbook?
The label Latin American generally refers to people who live in Central American countries. Although Spain colonized much of what is now South and Central America and parts of the Caribbean, the inhabitants of these areas are now much more diverse. Depending on the region or country, some people primarily trace their lineage to the indigenous people who lived in these areas before colonization, or to a Spanish and indigenous lineage, or to other combinations that may include European, African, and/or indigenous heritage. Latina and Latino are labels that are preferable to Hispanic for many who live in the United States and trace their lineage to South and/or Central America and/or parts of the Caribbean. Scholars who study Latina/o identity often use the label Latina/o in their writing to acknowledge women who avow that identity label (Calafell, 2007). In verbal communication you might say “Latina” when referring to a particular female or “Latino” when referring to a particular male of Latin American heritage. When referring to the group as a whole, you could say “Latinas and Latinos” instead of just “Latinos,” which would be more gender inclusive. While Hispanic is used by the US Census, it refers primarily to people of Spanish origin, which doesn’t account for the diversity of background of many Latinos/as. The term Hispanic also highlights the colonizer’s influence over the indigenous, which erases a history that is important to many. Additionally, there are people who claim Spanish origins and identify culturally as Hispanic but racially as white. Labels such as Puerto Rican or Mexican American, which further specify region or country of origin, may also be used. Just as with other cultural groups, if you are unsure of how to refer to someone, you can always ask for and honor someone’s preference (Communication in the Real World. 2016).
Since the early 1900s, Latinos have been a productive and essential part of Minnesota. Most of the earliest Minnesotanos were migrant farm workers from Mexico or Texas and faced obstacles to first-class citizenship that are still being addressed. They overcame the instability associated with migratory work by establishing stable communities in the cities and towns of Minnesota. Latinos faced, and still face, discrimination—both racial and the kinds common to all immigrants and migrants.
To overcome these obstacles, Latinos built institutions—from churches to unions to arts collectives to service organizations like CLUES and the LEDC—designed to create spaces for survival and organizing for first-class citizenship. The spread and success of these institutions have allowed for consequential organizing by Latinos for a visible and powerful place in Minnesota.
Who are Latino and Latina Minnesotans? They are people with roots in Latin America—from many nations and with different experiences—who came to form an identity shaped by migrations, immigration, and struggles for first-class citizenship. Latino is a contested term and is best understood as an ongoing negotiation among the different groups that claim it.
Since about one-third of the United States was once part of Mexico, many Latinos can trace their U.S. citizenship back to 1848, some ten years before Minnesota became a state. With the exception of Puerto Ricans, who are U.S. citizens by birth, there is considerable diversity of citizenship within all the other national groups that make up the category.
In 2013, about 60 percent of Latinos in Minnesota were born in the United States. Indeed, many Latino families have within them people with different immigration status. Differences in religion, language, gender, sexuality, race, and class make Minnesota’s Latinos a rich and complex community. By far the largest and most established group of Latino Minnesotans is of Mexican heritage (70 percent). The next largest groups are from Puerto Rico (about 4.3 percent), Ecuador and El Salvador (2.9 percent each), and Guatemala (2.7 percent).
Key Points and Chronology from The MN Historical Society
Mexican and Mexican-heritage workers began working in Minnesota in the early years of the twentieth century, primarily as migrant farm laborers. In the 1920s, permanent Latino urban settlements emerged in the Twin Cities, with the West Side of St. Paul serving as the main settlement. Members of the Mexican community, sometimes with allies, established institutions whose spaces helped them survive and carve out a space in Minnesota.
1886 Luis Garzón settles in Minnesota, where he will become a significant leader of early Mexican migrants and immigrants.
1900s A twenty-year period of migratory farm work, primarily in the sugar beet industry, begins. This labor comes to dominate Latino life in the state.
1920s Urban settlements on St. Paul’s West Side Flats and East Side; in Minneapolis; and in Inver Grove Heights begin to form. From these, a permanent place develops for Minnesota Latinos to start their lives in the state.
1920s Mexican migrant workers come to Minnesota to work on sugar beet farms.
1922 The Anáhuac Society is established and provides a solid foundation for Latinos to survive in a new environment, as well as an institutional basis for organizing.
1930s Migrant workers looking for permanent homes cause a housing shortage. They begin to form an enclave on St. Paul’s West Side.
1931 At least 15 percent of the Mexican settlement in St. Paul is repatriated (forcibly removed) to Mexico.
1931 Our Lady of Guadalupe Mission is founded in St. Paul. It becomes a central place for spiritual refuge and community organizing.
1942 The Mexican Farm Agreement of 1942, also known as the Bracero program, creates a temporary-worker program between the Mexico and United States that alleviates the labor shortage created by World War II.
1943 Minnesota employers began to participate in the Bracero Program, which imported contact Mexican labor to help with the agricultural production throughout the state. Participation continued until 1964.
1947 The federal legal case of Mendez v. Westminster Supreme Court determines that schools cannot not segregate Latino children from white children in classrooms, a major achievement for the Chicano movement.
1952 Flooding causes the evacuation of 2,741 residents from Westside St. Paul.
1954 An industrial park is completed in Westside St. Paul at a total cost of $13 million.
1954 The U.S. Supreme Court’s decision in Hernandez v. Texas extends Fourteenth Amendment rights related to citizenship and equal protection of laws to people of all races.
1957 A second severe flood forces many Latino families to move to new housing built near the industrial park.
1960 The West Side Flats in St. Paul are destroyed as part of an urban renewal project. Their removal disrupts the heart of the Latino community and helps give rise to the local Chicano Movement.
1964 The Braceros Program ends.
1965 The five-year-long Delano Grape Strike begins, and Minnesotans join the national boycott.
1966 Sister Mary Giovanni Gourhan proposes the Guadalupe Area Plan, designed to address the opportunity gap for Mexican residents through alternative education centered on their heritage.
1967 A Minnesota chapter of the Brown Berets forms in St. Paul.
1969 The first of a series of protests at the University of Minnesota is held. The protests lead to the establishment of the Chicano Latino Studies Department.
1969 On February 19, Cesar Chavez begins a twenty-five-day hunger strike in order to bring national attention to the mistreatment of agricultural workers.
1972 The Minnesota Brown Berets disband.
1977 Conrado “Conrad” Vega becomes the first Latino to serve in the Minnesota Legislature.
1977 Comunidades Latinas Unidas en Servicio (CLUES) begins to organize. The social services provider has since become one of the leading institutions for Latinos in the state.
1978 The Chicano Latino Affairs Council is created as an official state agency to advise the governor and the legislature on issues of importance to the Latino community.
1995 St Cloud State University students carry out a hunger strike to establish a Chicano/a Studies program and improve conditions for Latino students, faculty, and staff.
1998 Edwina Garcia becomes the first Latina elected to the Minnesota Legislature.
Cultural Atlas and Mexican Culture
While the following country description and communication descriptions with Do’s and Don’ts are written about Mexican culture, not Mexican-American culture, we are sharing this information from Cultural Atlas to give students a more in-depth overview. According to the Cultural Atlas (and shared with written permission):
“Mexico is a North American country bordering the United States, Guatemala and Belize. It is extremely geographically diverse, with deserts, high mountain plateaus and tropical coastlines. More than half of the Mexican population lives in the central regions of the country, whilst the arid north and tropical south are more sparsely populated. The dominant culture of Mexico reflects a blend of indigenous and Spanish customs; however, traditions vary greatly across the country. Many of the things often thought of as distinctively ‘Mexican’ have a local or regional origin. For example, tequila, mariachi music, embroidered sombrero and costume of the charro (gentleman rancher) originated in the west of Mexico. Each region/state generally has a unique cultural identity and accompanying cuisine, folk songs and craftsmanship that residents are very proud of. Cultural customs may also vary on a more local level, between communities, towns and cities within states” (Cultural Atlas, 2021).
Mexican Cultural Communication Descriptions
Attribution: The primary author of this profile was Nina Evason (2018) the materials are shared on the Cultural Atlas.
Verbal Communication
Indirect Communication: Mexicans are generally indirect communicators. They rarely give direct refusals or deliver delicate information in a blunt way. This is considered impolite. Instead, they tend to take a long-winded, roundabout approach to convey their messages sensitively and tactfully to avoid conflict or confrontation.This involves using gentler, more diplomatic expressions to provide a negative answer in a more sensitive way. For example, they may say they will “see what I can do” instead of giving a straight “no.”
Refusals: Mexicans can be quite hesitant to give direct refusals. This can mean that they agree to do something they do not want to (or cannot do) in order to avoid sounding rude. If you ask a question that requires a direct ‘yes’ or ‘no’ answer, your Mexican counterpart may take some time talking inconclusively before reaching their answer. This is intended to soften the words. Furthermore, if you receive a final answer that is unsettled (e.g. “maybe”, “let’s wait and see” or “let me think about that”), it is a generally a good indicator that they mean “no.”
Language Style: When speaking in Spanish, Mexicans use a lot of diminutives to convey their meaning in a softer or more affectionate way. This is usually done by adding ‘ito‘ or ‘ita‘ to the end of a word. For example, they may refer to their “abuelo” (grandfather) as “abuelito” (meaning ‘grand pappy’), or they may say that a man is “thin on top” (calvito) instead of “bald” (calvo).
Slang: It is common to hear Mexicans say ‘Güey‘ at the end of a sentence when talking to friends or those of the same status. This is a casual phrase that is the close equivalent of ‘dude’ in English. For example, one might say “Si güey” meaning “Yeah dude”.
Formality: There are different forms of expression in Spanish that communicate varying levels of courtesy and formality. The polite form of speech is to address people in the formal form of ‘you’ (known as ‘usted‘). This should be used when addressing anyone of a higher status out of respect. The informal ‘you’ (known as ‘tú‘) is generally used between people who know each other very well and among the youth.
Inverted Question Marks: In the Spanish language, questions are written with an inverted (or upside-down) question mark at the beginning of the sentence. For example: ¿Cuántos años tienes? (How old are you?).
Groups: In casual social situations, Mexicans may talk over one another and allow their laughter to grow very loud. In these settings, it is generally acceptable to interrupt to be heard and join in with similar enthusiasm.
Nonverbal Communication
Physical Contact: Many Mexicans are generally very tactile people. Open displays of affection between couples are common and acceptable. Among friends, people may nudge your arm, elbow or leg to reinforce their points in conversations, put an arm around your shoulder in camaraderie or hold both your shoulders to show deep appreciation. Some people may even casually finger the lapel of another person’s clothing, or neaten their attire for them. All these moments of physical interaction are meant to signify friendly affection and approachability.
Personal Space: Mexicans typically stand quite close to each other while talking. Maintaining too great a distance from another person can be seen as unfriendly or standoffish.
Eye Contact: Direct eye contact is expected and appreciated. Sometimes Mexicans may hold your gaze for a prolonged period. This is normal and is not meant to imply any particular connotation other than interest and sincerity.
Body Language: Mexicans tend to use many hand and arm gestures throughout the conversation. People belonging to indigenous groups tend to have a particularly reserved and shy demeanour around foreigners or urban Mexicans.
Gestures: Mexicans communicate “yes” by holding their index finger up (as if to point) and then curling it up and down repeatedly and quickly. People may indicate “no” by shaking the hand from side to side with the index finger extended and palm facing outward. People may gesture to ask for you to share something or give a piece (mochate) by making a chopping motion on their forearm.
Nodding: Be aware that some people may nod out of respect for what you are saying. It does not always indicate agreement with one’s words
Cultural Atlas’ Advice for Do’s and Don’ts of Mexican Culture
As a reminder, this information is shared in the aggregate. Mexican-Americans spread throughout the United States may identify more with their regional identity of being a New Yorker, a Midwestern, a “Tex-Mex” personal, or a Californian. “Dos and Don’ts” from those with Mexican heritage living elsewhere and within Mexico itself.
Activity Idea: ask our class guest speakers if they agree or disagree with the information below. What might they add?
Do’s
Be respectful and courteous, especially when in the company of parents or elders.
Try and be open to the friends and family of your Mexican counterpart. Mexicans are often very welcoming to friends of friends on the basis of small social connections. They will appreciate it if you are similarly open-hearted to their loved ones.
Refer to Mexican migrants living in the U.S. without paperwork as “undocumented migrants”. Avoid using the term “illegal”.
Have an understanding of Mexico’s cultural achievements and mention them when you see fit.
Try and offer your service to help with domestic duties or basic tasks whenever possible. Even if a Mexican declines your offer, it is polite to extend the gesture.
Be sure to thank Mexicans for their hospitality. It is the only gesture expected in return for their generosity.
Share stories from your country, home and family life. Mexicans love tales from other parts of the world.
Don’ts
Never criticise the Virgin of Guadalupe or say anything about her that could be perceived as a slight (see ‘Catholicism in Mexico’ under Religion).
Do not stereotype Mexicans as ‘narcotraficantes‘ (drug traffickers) or heavy drug consumers. Only a very small percentage of the population is engaged in such activity. Furthermore, consider that the current violence of cartels is driven by the Western consumption of drugs. Meanwhile, the Mexican consumption of illicit drugs is lower than U.S. levels.1
Do not emphasise Mexico’s problems or seek to make people feel ashamed of them. Most Mexicans are disgusted by violence and want to redeem the reputation of Mexico in foreigners’ eyes. Furthermore, while they are very critical of their own nation’s issues, they do not need further judgement from outsiders – especially when this criticism is informed by stereotypes.
Do not criticise another person in public, or in earshot of others. Deliver all sensitive news privately to avoid embarrassing others.
Avoid referring to the United States as “America”. Mexico is also a North American country and some people can find it frustrating when the term is used solely to refer to those from the USA. Therefore, Mexicans may call Americans’ estadounidense’ instead of ‘americano‘ in Spanish.
Do not imply that Mexicans are overcrowding the U.S. or flooding the U.S. border with undocumented immigration. In reality, the numbers of Mexican migration has been steadily declining.2
Do not imply that Mexicans are lazy. The population works more hours on average than any other OECD nation.3
_____________________
1 U.S. Department of State, 2016
2 Pew Research Centre, 2015
3 OECD, 2018
Cultural Atlas’ Advice for Greetings in Mexico
As a reminder, this information is shared in the aggregate. Mexican-Americans may differ in communication style, Greetings, and Dos and Don’ts from those with Mexican heritage living elsewhere and within Mexico itself.
Activity Idea: ask our class guest speakers if they agree or disagree with the information below. What might they add?
Greetings
A firm handshake with eye contact and a smile is the appropriate greeting in most situations. In more casual settings, people may simply give one another a nod of the head.
Once people become acquainted, greetings become a lot warmer and Mexicans often prefer to embrace (abrazo). This involves a loose embrace accompanied with a kiss on the right cheek.
The common verbal greeting is “Buenos dias” (Good day), “Buenas tardes” (Good afternoon) or “Buenas noches” (Good evening/night) depending on the time of day.
A more casual greeting is “Hola” (Hello), “¿Qué tal?” (What’s up?) or “¿Cómo estás?” (How are you?).
Be aware that greetings may differ in predominantly Indigenous towns. For instance, in many towns in the state of Oaxaca, the expected greeting is a loose handshake (never a kiss or embrace) as close physical contact with people outside of one’s family is less common.
It is generally polite to show personal interest in the person you are greeting, such as enquiring about their family and health.
The formal title used to greet people is ‘Señor‘ (Mr) for men and ‘Señora‘ (Ms) for women. This is followed by one’s surname.
Elders may be addressed as ‘Don‘ (Sir) or Doña (Ma’am) followed by their first name to show more respect.
It is common for people to briefly interrupt a conversation in order to greet somebody who has just arrived or who is passing by. This is generally not considered rude.
Attribution for Cultural Atlas: Mexico
Cultural Atlas. (n.d.). Mexican culture. Cultural Atlas. Retrieved December 20, 2021, from https://culturalatlas.sbs.com.au/mexican-culture
Section Two: Medial and Dental Case Study
Section Two – Medical & Dental Case Study Learning Outcomes
When you have completed this section of the chapter you should be able to do the following:
Compare and Contrast Medical and Dental care in the US and Mexico (watch the linked videos)
Apply Hofested’s Theory to the Case Study of Medical/Dental Care
*Understand the diverse issues of healthcare practices
*Explain some of the cultural issues within effective healthcare
*Explore the variety of healthcare options
*Discuss how religion, power, ethics, and identity impact healthcare
*Discuss how culture impacts the ethical implications of healthcare (*last five learning outcomes are attributed to Karen Krumrey)
The following links can not “embed” into our PressBook – you will find them in D2L – please link to them and watch how Fredy explains dental care (and medical care) in his home country of Mexico. He is studying at RCTC to complete his nursing degree. Fredy was a student in Intercultural Communication with Lori Halverson-Wente in 2021, the height of COVID. Fredy’s interview was conducted with RCTC’s Dental Hygiene instructor Katie Ristau and Spanish Instructor, Lillyam Arroyave (Lillyam.Arroyave@rctc.edu). We have combined Fredy’s and Lillyam’s interview with materials previously published on intercultural communication and Medical Care shared generously from Karen Krumrey as noted above.
“The Human Genome Project (1990-2003) identified 20,000-25,000 genes in human DNA making it possible to efficiently tackle more health-related problems than ever before. What the Human Genome Project couldn’t study though was the effect of culture on healthcare. We have learned that effective intercultural communication can mean increased profits or opportunities in many contexts, but in the healthcare setting, effective intercultural communication can impact a patients’ physical or mental well-being (Voelker, 1995), as well as their quality of life. This chapter is designed to introduce the complex issues that culture has on both the providers and receivers of healthcare around the world” (Krumrey, 2022).
In this week’s discussion, you’ll find an interview with Fredy and Lillyam where they discuss how Latino cultures shares, even though they are from different countries (Mexico and Colombia), high power distance compared to the United States. Lillyam further explains that in high-power cultures, the patient is much more likely not to question authority. That means, she explains, that if the Dentist says we need to pull a tooth, the patient has historically agreed and not questioned the dentist in high-power countries. The Hofested Insights website describes Power Distance: “This dimension deals with the fact that all individuals in societies are not equal – it expresses the attitude of the culture towards these inequalities amongst us. Power Distance is defined as the extent to which the less powerful members of institutions and organisations within a country expect and accept that power is distributed unequally. At a score of 81, Mexico is a hierarchical society. This means that people accept a hierarchical order in which everybody has a place and which needs no further justification. Hierarchy in an organization is seen as reflecting inherent inequalities, centralization is popular, subordinates expect to be told what to do and the ideal boss is a benevolent autocrat” (2022).
Hofsted Insights further shares how collectivist countries often find a “moral” component to decisions. To not follow an esteemed person in power, like a Dentist or Doctor, would be shunned upon. As Fredy shares, too, seeing a doctor or dentist when he was growing up was a rare occasion. “Mexico, with a score of 30 is considered a collectivistic society. This is manifest in a close long-term commitment to the member ‘group’, be that a family, extended family, or extended relationships. Loyalty in a collectivist culture is paramount, and over-rides most other societal rules and regulations. The society fosters strong relationships where everyone takes responsibility for fellow members of their group. In collectivist societies offence leads to shame and loss of face, employer/employee relationships are perceived in moral terms (like a family link), hiring and promotion decisions take account of the employee’s in-group, management is the management of groups.” (Hofsted Insights, 2022).
The screenshot below will link you to the full data:
Patient and Diversity Issues
*the materials below were written and attributed to Karen Krumrey (2022).
The US has one of the most diverse societies in the entire world. There are residents and visitors from almost every place on the planet therefore US healthcare must be approached from a multi-cultural perspective. Doctors face effective communication issues, trying to understand the various cultural and co-cultural issues, and the reality that accessible care might not be available to all patients. Patients face language issues, lack of knowledge of healthcare and treatment options, and historical treatment within healthcare systems.
Language Issues
Healthcare professionals often use medical terminologyor jargon. Medical terminologyis the scientific language used by doctors to describe specific medical conditions. Examples of medical terminology could be thrombosis for a blood clot and hypertension for high blood pressure. Jargon is often the shorthand used between people practicing the same profession and it might have no meaning outside the profession. Examples of jargon in the healthcare world would be BP for blood pressure, NPO (nil pers os) or nothing by mouth, and c-section for birth by caesarian section.
Another issue is that healthcare providers and patients may both operate out of an ethnocentric framework without realizing it. Cultural beliefs and the ensuing approaches to healthcare are so fundamental to a human being that they are not often overtly communicated, but rather just assumed. For instance, people from different cultures do not always report pain in the same ways, which easily leads to miscommunication in cross-cultural encounters (Lee et al., 1992) and the assumption that some cultures do not feel pain. In working with patients from other cultures, healthcare providers can learn as they go, but this has the potential to be dangerous when dealing with diagnosis and treatment of issues.
Cultural Beliefs Influence Healthcare
Today 60 million US Americans (nearly 1 in 5) speak a language other than English at home and of that 60 million, 25 million self-identify as not speaking well (CM Elearning, 2022). Finding adequate translators and interpreters who are familiar with medical terminology is difficult. There is plenty of evidence that gaps in translation can lead to adverse outcomes, but one thing is even more clear, patients can’t make decisions about treatment without a competent medical translator. As more of the patient’s family and friends’ attempt to translate, there is more potential for harm than good.
And lastly, treating patients is not always a matter of communication just between doctors and patients. Most cultures have laws regarding healthcare issues and practices. In the United States the judicial issue of informed consent requires that all patients receive full information enabling them to freely make decision about their own health care (Gostin, 1995). This might make sense to you, but in some family-centered cultures, this might be a problem. In this case, families and extended families may expect to be actively involved by providing input and support on treatment decisions.
Photo – Translator anyone?
Historical Treatment of Cultural Groups
Widespread stereotypes and prejudice directed toward different cultural groups have fostered differential treatment for some groups—especially racial and ethnic minorities. Some historical examples that you might be familiar with are Josef Mengele, the SS physician at Auschwitz, Germany who conducted experiments on Holocaust prisoners that included giving prisoners infections to watch the progression of the disease and spraying them with chemicals to test possible chemical warfare solutions.
Photo: Josef Mengele, Auschwitz
In the 1930s and 1940s, Japan’s Imperial Army Unit 731 conducted biological warfare and medical testing on Chinese civilians. As many as 200,000 people were impacted. There were also the Asian “comfort women” of World War II. The term comfort woman is a euphemism for women that were captured and forced to work in brothels. Many experienced great cruelties without access to medical care.
Photo: Comfort Women Rally in Seoul, Korea
Of course, in the United States, there was the Tuskegee Syphilis Project that lasted for 40 years (1932-1972) in which researchers conducted a study on the health effects of untreated syphilis. African American men who enrolled in the “project” were told that they were being treated for “bad blood.” During the same time, the US was also doing experiments with syphilis in Guatemala on prisoners and individuals with mental illness. Based on both recent and historical atrocities, it is not surprising that some cultural groups are suspicious of healthcare.
Figure 12.5 – Participants in the Tuskegee Syphilis Project
Prejudicial ideologies or sets of ideas based on stereotypes, can cause significant barriers to intercultural communication, and may influence the quality of care that patients receive. Patients may enter the healthcare system with their own prejudices based on historical events, distrust of doctors, distrust of certain treatments, and more. Professional healthcare workers may lack an understanding of healthcare provided outside of the traditional western system and that are a part of cultural traditions other than their own.
Cultural Differences in Healthcare Concepts
Health is a cultural concept. Culture frames and shapes how we perceive the world, and our experiences, hence different cultures bring different perspectives on health. Most cultures fall somewhere within the individualism and collectivism continuum. Verbal communication styles that directly affect health care are traits like direct/indirect communication, high/low context, and honesty versus harmony. Nonverbal communication styles would include high and low contact. Healthcare is also heavily impacted by the cultural view of power relationships.
Photo -Healthcare, Not Wealthcare! rally in Philadelphia
Culture helps to define what patients and healthcare providers believe about the causes of illness, which diseases are stigmatized and why, how illness and pain are experienced and expressed, where patients seek help and ask for help, and the acceptance of a diagnosis (Mayhew, 2018). Please remember that as significant as culture can be, within any given culture, there will be variations among individual members.
Belief Systems
The healthcare process is often represented through different worldviews that we commonly call Eastern and Western medicine. Eastern medicine describes a disease as a signal that the body is out of balance. Instead of viewing illness as something to cure, Eastern medicine uses natural plants to work with the natural process of the body. Western medicine on the scientific method to understand what causes illness. For many, human beings are just like “machines” that need fixing or tuning to “eradicate the enemy” (Todd, 1999).
In the US, and other nations that practice Western medicine, the dominant healthcare model is based on biomedical science. According to the biomedical method, doctors look for physical signs of what is wrong. Once the symptom is identified, things like drugs and procedures are used to get rid of the problem. Providers who operate from a biomedical model, might communicate in ways that are efficient and logical. This approach uses relatively little time, and providers might see many patients in a day.
Photo – Biomedical Model
In nations that practice Eastern medicine, the dominant healthcare model is biopsychosocial. The biopsychosocial model acknowledges that illness is not always just a physical thing. Disease and illness are often influenced by environment and social factors as well as emotions, stress, and lived experiences. Patients and providers may care deeply about communication and the “bigger picture” which often means spending significant amounts of time working through the illness together.
Alternative Medicine
Healthcare provided outside the traditional Western medicalsystem to Westerners is often referred to as “alternative medicine”whether they fall within the Eastern medicalsystem or not. Alternative medicine can mean returning to traditional cultural medicinal practices such as herbal remedies and sweat lodges, or it can also mean seeking out medical practices that are part of other cultural traditions rather than your own such as acupuncture and cupping.
Alternative medicine generally falls into four broad categories:
The first is referred to as mind-body medicine which focuses on using the mind to influence the body. These types of approaches might include patient support-group therapy, meditation, and prayer.
The second is biologically based practices which refers to the use of products found in nature. These types of approaches include the use of herbal therapies, dietary supplements, and other natural products.
Photo -Herbs at Medicinal Plants and Traditional Medicine exhibition in Iran’s capital.
The third category would be manipulativeandbody-based practices. This approach refers to the use of massage or chiropractic manipulation to promote health.
And the last type is referred to as energy medicine which could include acupuncture, Reiki, and certain types of massage.
Photo -Acupuncture
Social Implications of Illness
The ways that a culture perceives health is influenced by different things in a culture. Social implications can be defined broadly such as climate and environmental factors, but there can also be more specific factors such as emotional, economic, family, and community factors that impact patients.
Diseases often carry their own emotional stigma within a culture. HIV, cancer, alcoholism, drug addiction, and mental illness can cause both patients and family members to feel shameful and withdraw from treatment and cultural interaction.
In countries without [insurance options,] universal or nationalized healthcare systems, health costs can economically devastate families, cause family members with employer provided insurance to be underemployed to avoid losing insurance, or impact credit ratings and job opportunities. Poor people can feel that they have no control over health problems and fatalistically make bad choices.
Photo – HIV/AIDS Patient in Hospital.
The impact of disease on the families of patients is often unrecognized and underestimated. Family members are often care givers as well as economic providers. Much has been studied about quality of life issues for family members and chronic illnesses cross cultural boundaries although in some families’ relationships can grow stronger as members work together.
Much has also been studied about community interaction as well. Community interaction can range from “drifting away” to ostracism and fear of stranger’s reactions to community organization of support.
Religion and Healthcare
When people become ill, and the treatment isn’t effective, some people are driven to seek answers to questions from sources outside of the science-based medicine process. The role of religion and spirituality in healthcare raises several issues about ethical ways to incorporate healthcare practices into existing beliefs. Some providers worry about religious freedom issues, while others may not be aware of the diversity of religious beliefs surrounding health care.
Photo – Hospital Chapel
Religious beliefs can impact concerns about modesty and being treated by someone of the opposite sex. Some patients will refuse to consume certain foods or eat at certain times or even take medications that are produced using problematic processes. Pain medications may be welcomed or shunned because of beliefs. Healthcare providers may also be asked to minimize actions that might disturb the sick person. Washing, fasting, jewelry might have to be negotiated with providers. Other points of negotiation might be blood and organ donations, transplants, withholding or providing life-sustaining therapy, and the burial of amputated limbs. Family and faith community members might expect to keep company with a dying patient, and for some the bodies of the dead may have to be buried or cremated as soon as possible. And it cannot be stressed enough that rituals and prayers occur in a variety of different ways, but they are all viewed as a necessary part of the healthcare process.
Learn a bit more…
While religious and spiritual beliefs may vary, there are strategies for helping healthcare professionals serve religious patients. The following is a compilation put together from lists provided by the Agency for Healthcare Research (2015), the US Health Resources & Services Administration (ret. 8/10/19), the University of Pennsylvania Medical System (2008), the University of Washington Medical Center (1997), and the Canadian Paediatric Society (2019).
Help patients feel comfortable at the facility.
Establish a relationship with patients by supporting or encouraging religious beliefs.
Provide health information in ways the patient accepts.
Maintain good communication with patients
What do you call your illness and what do you think caused it?
Is there anything I should know about your culture, beliefs, or religious practices that would help me take better care of you?
Do any traditional healers advise you about your health?
Do you have any dietary restrictions that we should consider as we develop a food plan?
Your condition is very serious. Some people like to know everything that is going on with their illness, whereas others may want to know what is most important but not necessarily all the details. How much do you want to know? Is there anyone else you would like me to talk to about your condition?
Show patients respect by viewing religious and spiritual support as part of the healthcare plan.
Be ready for when religious and spiritual support are not available.
Power and Ethics in Healthcare
Healthcare is ripe with imbalances in power. Providers and patients are not equal in medical knowledge, nor can patients access treatment procedures without referral from a provider. Patients may encounter many healthcare workers within a short amount of time without knowing why or how they are related to treatment. Questions may be seen as a challenge to authority.
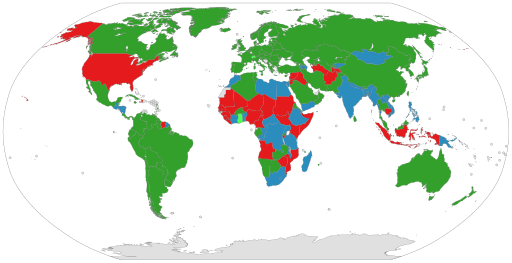
In the United States, healthcare is a business. It’s a HUGE business. Deloitt.com (ret. 8/11/19) estimates an annual growth rate of 5.4% between 2017 and 2022. In dollars this is 7.077 trillion in 2015 to 8.734 trillion in 2022. The insurance industry drives MOST healthcare decisions in the US. Costs impact how the US thinks about medical resources and their distribution. For people who come from other healthcare systems, the private healthcare system as practiced in the United States can be confusing or downright inaccessible.
Photo – Universal Healthcare by Country
Ethics
The insurance industry and the fear of malpractice suits guides many decisions regarding medical ethics in the United States. Some healthcare organizations use ethics committeesstaffed by healthcare professionals, religious leaders, social workers, and governmental agencies to help make decisions about medical ethics. Such committees could debate about providing or discontinuing care for terminally ill patients and the possible funding of drug rehabilitation programs for a long-term drug addict. If there are value-laden or value-dependent questions that go beyond what medical science can address, but there is a need for a decision to be made, the issue is most often referred to an ethics committee (Aulisio, 2016).
Photo – Ethics Committee
In the US, the ethics committee rose into prominence during the 1962 through 1990 time period (Aulisio, 2016). In Eastern and Central Europe, ethics committees were the result of fundamental political and societal change during 1989-1990. Whereas in Western Europe, ethics committees were common at the local level, but didn’t become nationalized until the early 2000s (Steinkamp et. al, 2007).
Some medical procedures are very controversial, even among members of the same culture. In the United States, abortion, and euthanasia, or assisting terminally ill people in committing suicide, are two prime examples. As a state, Oregon is often required to defend its ‘Death with Dignity Law’ from interest group lawsuits.
Photo – – Holding a dying grandmother’s hand
Information-Sharing, and Identity
Knowing the appropriate way to communicate with families and patients in an intercultural context can be incredibly complex. In some cultures, the family is involved in the healthcare and medical treatment of its members. In other cultures, medical information is confidential and only given to the patient. Some patients may not want their families involved in their care if they have had a miscarriage, are suffering from certain types of cancer, or are depressed. All patients will act within a framework of cultural values.
Information Sharing
In general, healthcare providers will give information regarding patient health in four general frameworks.
Strict Paternalism – reflects a physician’s decision to provide misinformation to the patient when he or she believes it is in the best interests of the patient.
Benevolent Deception – occurs when the physician chooses to communicate only part of a patient’s diagnosis.
Contractual Honesty – refers to the practice of telling the patient only what he or she wants to hear or to know.
Unmitigated Honesty – refers to when a physician chooses to communicate the entire diagnosis to a patient. (Martin & Nakayama, 2007)
In the United States, unmitigated honesty is the only one of these options that is legal for adults. When seen as too difficult or frustrating, cultural, and legal differences between provider and patient can contribute to a patient’s inability to understand the provider’s directions. Communication problems resulting from conflicting identities and perceptions can be overcome with sensitivity and adaptation (Brown & School, 2006).
Identity
Both patients and providers are concerned about their cultural identities. Communication Theory of Identity (Hecht, 2009) explains that people make assumptions about each other based on their backgrounds. The premise behind this theory can help to explain how misunderstandings occur in the intercultural healthcare setting (School, Wilson, & Hughes, 2011). Individuals use their identities to affiliate themselves with groups and cultures. The extent to which people identify with specific groups and cultures varies based on the dimensions of salience and intensity (Hecht et al., 1993).
Identity salience refers to the fact that people view their cultural identity as an important part of who they are, while identity intensity refers to the level of importance that people place on their cultural identity (Brown, 2006). When people from different cultures interact, they communicate according to the ways that people from their culture communicate, and by doing so, enact their identity with particular groups.
Hecht (1993) asserted that there are four frames that may overlap and occur in the same communicative interaction: personal, enactment, relational, and communal. Each identity frame has its own set of assumptions concerning how the intercultural provider-patient interaction negotiates identity (Brown, 2006). In a 2017 study on intercultural healthcare communication through the eyes of patients in the Netherlands, Patternotte et. al, found that a doctor’s cultural background was not important if the doctor was a professional, but noted that all of the patients had already lived in the Netherlands for a significant amount of time. Some patients did have a clear preference for a doctor of a particular gender. Many patients felt that a competent doctor needed to be accessible, have enough time, treat them as unique people, and ask about cultural habits. Respect for cultural identity was an integral part of communication skills in a healthcare setting.
Conclusion of this Case Study
Communication is vitally important to the competent functioning of healthcare services. Patients and providers may not be satisfied with their healthcare interactions when they do not communicate effectively with one another. Although this chapter has just skimmed the surface of a vast and complicated topic, a knowledge of intercultural communication theories and skills can be the beginning of competence and success in the healthcare arena.
Key Terms For the Case study
Medical Terminology
Eastern Medicine
Biopsychosocial Model
Biologically Based Practices
Strict Paternalism
Unmitigated Honesty
Communication Theory of Identity
Jargon
Western medicine
Alternative medicine
Body-Based Practices
Benevolent Perception
Euthanasia
Identity intensity
Prejudicial ideology
Biomedical Model
Mind-body Medicine
Energy Medicine
Contractual Honesty
Identity Salience
Suggested Reflection Questions
Why might people in the United States seek out alternative forms of health care such as acupuncture?
How might intercultural communication misunderstandings arise between patients, their families, and health care professionals? Provide an example.
What medical jargon have you encountered in your interactions with health care professionals? Did it effect your communication? If so, how?
What are some examples of power imbalances in the health care interaction?
If you were suffering from a disease, which ethical framework (strict paternalism, benevolent deception, contractual honesty, or unmitigated honesty) would you want your health care professional to use when communicating with you and your family? Why?
Section Three- Minnesota Resources and A Final Case Study in St. Paul
A Final Case Study: Chicano Movement in Westside St. Paul
Written by: Shirley Saldivar
Biography: Shirley Saldivar graduated from the University of Minnesota in 2016 with a degree in history. She was a History Museum Fellow at the Minnesota Historical Society in 2016.
First published: May 15, 2019 | Last modified: July 22, 2021
When migrant workers from Mexico began to look for homes in Minnesota in the mid-twentieth century, many joined a growing enclave in Westside St. Paul. In spite of challenges, they sought opportunities to create a strong community and build a brighter future. They saw the Chicano Movement of the 1960s and 1970s as a means to that end.
During the 1960s, as the nation was experiencing a civil rights movement for African Americans, Mexican Americans were inspired to bring change to their own communities. They created the term Chicano to show a sense of pride, express resistance, and strengthen cultural identity. It was first used in Southern California and Texas, where Cesar Chavez, Dolores Huerta, and the United Farm Workers were uniting figures. Their political and social work came to be known as the Chicano Movement, or El Movimiento.
Mexican and Mexican American migration to the Midwest dates to the 1920s and 1930s, when laborers moved to the north to work on sugar beet farms. Over time, they set down roots in Minnesota communities—particularly St. Paul’s Lower West Side (the West Side Flats), which offered jobs in meatpacking and the railroad industry. Towards the end of the 1930s, so many Mexicans tried to settle near their families that there was a housing shortage in the neighborhood.
Much of the housing on the Lower West Side was eventually considered uninhabitable due to the area’s high risk of flooding. A flood in 1952 caused 2,641 residents to evacuate, and a second flood in 1957 emphasized a need for a long-term solution. The neighborhood had already become a target for urban renewal, and the St. Paul Port Authority had announced in 1956 that the Riverview Industrial District project would demolish the community. Families were reluctant to leave their homes, stores, schools, and churches, even though they were promised jobs in Riverview. The city completed the project in 1964 at a cost of $9 million for the construction and $4 million for relocation costs, but the jobs didn’t come in the quantity promised.
As a result of losing a section of their neighborhood, Mexicans and Mexican Americans took inspiration from the Chicano cultural movement happening throughout the United States. Some groups, including the U.S. government and southwestern Chicanos, disparaged the Midwesterners. The latter called them “culturally deprived” and claimed that they “didn’t know what it meant to be Chicano.” The comments, however, did not derail Chicanos in Minnesota, and they continued to seek connections and advice.
Sister Mary Giovanni Gourhan, a Westside St. Paul native active in Our Lady of Guadalupe Church, resolved to help her community specifically through education. In 1966, she came up with the idea of the Guadalupe Area Plan, also known as GAP. GAP was designed to fill the opportunity gap between Latino people and other groups through alternative education classes. The program admitted fourteen to nineteen-year-old students on probation or parole as well as those having difficulty in school.
GAP’s general school courses integrated Mexican history, culture, and tradition, creating an immersive experience for students intended to inspire pride in their work. They also built foundational skills for students to seek employment to provide for their families. By 1967, Gourham’s dream had become a reality, and GAP was a mainstay in the community. (In 2019, GAP continues to assist at-risk students via the St. Paul school system.)
In 1967, the Brown Berets, a pro-Chicano group, formed on the East Side of Los Angeles. Their objectives were to address police harassment, improve education, and increase political representation. A chapter was created in St. Paul in 1969. St. Paul’s Brown Berets served their community by raising funds for families in need, providing legal aid, and assisting the Guadalupe Area Plan by transporting craft goods.
There was also a push for Chicano history to be taught at the university level. In 1969, the University of California Santa Barbara’s Chicano Coordinating Council on Higher Education crafted a “Plan de Santa Bárbara”—a call to action to increase Latino recruitment, admission, representation, and programming in higher education. The Latin Liberation Front (LLF), a student group at the University of Minnesota, formed in 1970. On October 26, 1971, LLF students led by Ramona Rosales took over Morrill Hall and demanded that a Chicano Studies Department be created. The College of Liberal Arts agreed, and the first Chicano studies classes were held in the fall of 1972.
Attribution:
CiteSaldivar, Shirley. “Chicano Movement in Westside St. Paul.” MNopedia, Minnesota Historical Society. http://www.mnopedia.org/thing/chicano-movement-westside-st-paul (accessed December 7, 2021).
American Crystal Sugar Company Records
Manuscript Collection, Minnesota Historical Society, St. Paul
Description: Corporate records of the American Crystal Sugar Company, of its direct predecessor, the American Beet Sugar Company, and of other predecessors, subsidiaries, and affiliates. http://www2.mnhs.org/library/findaids/00341.xml
Film #A-64
Laughlin, Kathleen and Donald Morstad. Minnesotanos Mexicanos. Videocassette. St. Paul: Spanish Speaking Cultural Club Inc., 1978.
Audiovisual Collection, Minnesota Historical Society, St. Paul
Description: A documentary in which Minnesotans of Mexican heritage are shown in schools, at work, in religious and social environments, and in the political arena. Includes a brief history of Mexico up to the period (shortly after 1848) when Mexicans began migrating northward in their search for work. Emphasizes the importance of preserving the Mexican culture, which has existed in Minnesota almost 100 years. Also deals with contemporary issues such as bilingual education and migrant workers.
Lideres Latinos Oral History Project
Originally found at: http://collections.mnhs.org/ioh/index.php/10001458
Description : An essential oral history collection of Minnesota Latino leaders accessible as audio files or transcripts.
OH 49
Mexican-American Oral History Project, 1975–1976
Oral History Collection, Minnesota Historical Society, St. Paul
Description: In 1975 the Minnesota Historical Society began a two-year Mexican-American History Project under the direction of Ramedo J. Saucedo to collect the historical resources of this ethnic group: personal papers, records of organizations, photographs, articles, and other material, including 74 oral history interviews with people living throughout the state.
Project photographs, 1950s–1984
Housing and Redevelopment Authority of the City of St. Paul
State Archives Collection, Minnesota Historical Society, St. Paul
Description: Particularly well represented are individual residences, downtown blocks and views, individual commercial buildings, and urban renewal projects (demolition, house moving, project sites, and a few interiors of living quarters). http://www2.mnhs.org/library/findaids/gr00387.xml
Records of the Port Authority of the City of St. Paul, 1932–2012
State Archives Collection, Minnesota Historical Society, St. Paul
Description: The collection includes project files concerning Riverview Industrial Park (1893 and 1961–1962). http://www2.mnhs.org/library/findaids/gr01125.xml
Secondary
Vargas, Zaragosa. Proletarians of the North: A History of Mexican Industrial Workers in Detroit and the Midwest, 1917–1933. Berkeley: University of California Press, 1999.
Vega, Sujey. Latino Heartland: Of Borders and Belonging in the Midwest. New York: New York University Press, 2015.
Amato, Joseph. To Call It Home: The New Immigrants of Southwestern Minnesota. Marshall, MN: Crossing Press, 1996.
Arauza, Yolanda Lara. “The Settlement and Assimilation of Mexicans in Moorhead, Minnesota.” Master’s thesis, North Dakota State University, 2000.
Brownstein, M. (2019, July 31). Implicit bias. Stanford Encyclopedia of Philosophy. Retrieved April 26, 2022, from https://plato.stanford.edu/entries/implicit-bias/
Cultural Atlas. (n.d.). Mexican culture. Cultural Atlas. Retrieved December 20, 2021, from https://culturalatlas.sbs.com.au/mexican-culture
De La O, Gilbert. Interview with the author, November 15, 2018. Burrito Mercado, St. Paul.
Exploring Specific Cultural Identities. (2020, July 21). Butte College. https://socialsci.libretexts.org/@go/page/47450
Gibeau, Jane. “Not Funded; Classes Still Planned Sr. Giovanni Won’t Give Up.” Catholic Bulletin, January 7, 1966, 23.
Gonzales, Sandra M. “Aztlán in the Midwest and Other Counternarratives Revealed.” In Latinos in the Midwest edited by Rubén O. Martinez,17–31. East Lansing, MI: Michigan State University, 2011.
Holthaus, Gary. From the Farm to the Table: What All Americans Need to Know About Agriculture. Lexington, KY: University of Kentucky Press, 2009.
Lewis Dorothy. “Battling Nun: Wins Poverty Fund but Still Needs Equipment.” St. Paul Dispatch, May 13, 1966, 23-24.
Lopez, M. H., Krogstad, J. M., & Passel, J. S. (2021, September 23). Who is Hispanic? Pew Research Center. Retrieved April 25, 2022, from https://www.pewresearch.org/fact-tank/2021/09/23/who-is-hispanic/
López-Santamería, Maya. Música de la Raza: Mexican and Chicano Music in Minnesota. St. Paul: Minnesota Historical Society Press, 1999.
McClure, Jane. “A Story of Change, Pride, Perseverance: The Mexican-Americans and Their Roots in St. Paul’s Past.” Ramsey County History 27, no. 23 (Fall 1992): 4–12.
Muñoz, Carlos. Youth, Identity, Power: The Chicano Movement. London: Verso, 2007.
Saucedo, Ramedo J., comp. Mexican Americans in Minnesota: An Introduction to Historical Sources. St. Paul: Minnesota Historical Society, 1977.
Norris, Jim. North for the Harvest: Mexican Workers, Growers, and the Sugar Beet Industry. St. Paul: Minnesota Historical Society Press, 2009.
Rodriguez, Luis J. Always Running: La Vida Loca: Gang Days in L. A. New York: Touchstone, 2005.
Roethke, Leigh. Latino Minnesota. St. Paul: Minnesota Historical Society Press, 2009.
Rosario, Ruben. “Maria Lies Among Us.” St. Paul Pioneer Press, April 8, 2006.
Ruiz, Vicki L. From Out of the Shadows: Mexican Women in Twentieth-Century America. New York: Oxford University Press, 2008. First published in 1998.
Torres, Eden E. Chicana Without Apology. New York: Routledge, 2003.
Valdés, Dionicio Nodín. Barrios Norteños: St. Paul and Midwestern Mexican Communities in the Twentieth Century. Austin: University of Texas Press, 2000.
——— . El Norte: Agricultural Workers in the Great Lakes Region, 1917–1970. Austin: University of Texas Press, 1991.
——— . Mexicans in Minnesota. St. Paul: Minnesota Historical Society Press, 2005.
definition
"Personal identity is the way that we understand ourselves (e.g., personality, traits, and preferences) and is closely related to our concept of self."
“Our social identities are the components of self that are derived from involvement in social groups with which we are interpersonally committed” (Communication for the Real World, 2016).
Social identities differ from personal identities because they are externally organized through membership. Our membership may be voluntary (Maro is a member and leader in the group UNICOS MN) or involuntary (family), explicit (Marco pays a fee to continue to be a DACA member), or implicit (we purchase and listen to our favorite music genre).
"Cultural identities are based on socially constructed categories that teach us a way of being and include expectations for social behavior or ways of acting (Yep, G. A., 2002). Since we are often a part of them since birth, cultural identities are the less changeable [than social and personal identities]. The ways of being and the social expectations for behavior within cultural identities do change over time, but what separates them from most social identities is their historical roots (Collier, M. J., 1996)" (Communication in the Real World, 2016).
"Wildly held beliefs about a group of people" (Martin & Nakayama, 2022, p. 200).
"Implicit prejudice occurs at the unconscious level, is involuntarily formed and unknown to us."
Simply, to "pre-judge" a person, group of people, or society.
"Why do people hold prejudices? Psychologist Richard Brislin (1999) suggests
that just as stereotyping arises from normal cognitive functioning, holding prejudices
may serve understandable functions. These functions may not excuse prejudice, but
they do help us understand why prejudice is so widespread. He identifies the following
four such functions:
1. The utilitarian function. People hold certain prejudices because they can lead
to rewards. For example, if your friends or family hold prejudices toward certain
groups, it will be easier for you simply to share those attitudes, rather than risk
rejection by contradicting their attitudes.
2. The ego-defensive function. People hold certain prejudices because they don’t
want to believe unpleasant things about themselves. For example, if either of us
( Judith or Tom) is not a very good teacher, it will be useful for us to hold negative stereotypes about students, such as that they are lazy and don’t work hard.
In this way, we can avoid confronting the real problem—our lack of teaching
skills. The same kind of thing happens in the workplace: It is easier for people
to stereotype women and minorities as unfit for jobs than to confront their own
lack of skill or qualifications for a job.
3. The value-expressive function. People hold certain prejudices because they serve
to reinforce aspects of life that are highly valued. Religious attitudes often function in this way. Some people are prejudiced against certain religious groups
because they see themselves as holding beliefs in the one true God, and part of
their doctrine is the belief that others are wrong. For instance, Judith’s Mennonite family held prejudices against Catholics, who were viewed as misguided and
wrong. This may also be operating today as some U.S. Americans search for
validation of prejudices again Muslims. A more extreme example involves the
atrocities committed against groups of people by others who want to retain the
supposed values of a pure racial stock (e.g., “ethnic cleansing” by Serbs against
Muslims in the former Yugoslavia).
4. The knowledge function. People hold certain prejudices because such attitudes
allow them to organize and structure their world in a way that makes sense to
them—in the same way that stereotypes help us organize our world. For example, if you believe that members of a certain group are flaky and irresponsible,
then you don’t have to think very much when meeting someone from that group
in a work situation. You already know what they’re like and so can react to them
more automatically" (Martin & Nakayama, 2020 p. 203).
"Othering is a phenomenon in which some individuals or groups are defined and labeled as not fitting in within the norms of a social group. It is an effect that influences how people perceive and treat those who are viewed as being part of the in-group versus those who are seen as being part of the out-group.
Othering also involves attributing negative characteristics to people or groups that differentiate them from the perceived normative social group.
It is an “us vs. them” way of thinking about human connections and relationships. This process essentially involves looking at others and saying "they are not like me" or "they are not one of us."
Othering is a way of negating another person's individual humanity and, consequently, those that are have been othered are seen as less worthy of dignity and respect.
On an individual level, othering plays a role in the formation of prejudices against people and groups. On a larger scale, it can also play a role in the dehumanization of entire groups of people which can then be exploited to drive changes in institutions, governments, and societies. It can lead to the persecution of marginalized groups, the denial of rights based on group identities, or even acts of violence against others" (Cherry, 2020).
See: https://www.verywellmind.com/what-is-othering-5084425#:~:text=Othering%20is%20a%20phenomenon%20in,part%20of%20the%20out%2Dgroup.
This is a strong tendency to reflexively view one’s own cultural worldview, beliefs, and practices as superior to those of other cultures.
we seek out, conciously or unconciously, information that supports our stereotypes and ignores information that is inconsistent with our stereotypes (Grothe, 2021).
This dimension deals with the fact that all individuals in societies are not equal – it expresses the attitude of the culture towards these inequalities amongst us. Power Distance is defined as the extent to which the less powerful members of institutions and organisations within a country expect and accept that power is distributed unequally.
"a preference for a loosely-knit social framework in which individuals are expected to take care of themselves and their immediate families only" (Green, et al., 2018).
"Collectivism, represents a preference for a tightly-knit framework in society in which individuals can expect their relatives or members of a particular in-group to look after them in exchange for unquestioning loyalty. A society's position on this dimension is reflected in whether people’s self-image is defined in terms of 'I' or 'we' (Hofstede, 2012a)." (Green, et al., 2018).
A high score (Masculine) on this dimension indicates that the society will be driven by competition, achievement and success, with success being defined by the winner/best in field – a value system that starts in school and continues throughout organisational life.
A low score (Feminine) on the dimension means that the dominant values in society are caring for others and quality of life. A Feminine society is one where quality of life is the sign of success and standing out from the crowd is not admirable. The fundamental issue here is what motivates people, wanting to be the best (Masculine) or liking what you do (Feminine).
"The dimension Uncertainty Avoidance has to do with the way that a society deals with the fact that the future can never be known: should we try to control the future or just let it happen? This ambiguity brings with it anxiety and different cultures have learnt to deal with this anxiety in different ways. The extent to which the members of a culture feel threatened by ambiguous or unknown situations and have created beliefs and institutions that try to avoid these is reflected in the score on Uncertainty Avoidance."
(Hofstede Insights, 2022).
"This dimension describes how every society has to maintain some links with its own past while dealing with the challenges of the present and future, and societies prioritise these two existential goals differently. Normative societies. which score low on this dimension, for example, prefer to maintain time-honoured traditions and norms while viewing societal change with suspicion. Those with a culture which scores high, on the other hand, take a more pragmatic approach: they encourage thrift and efforts in modern education as a way to prepare for the future" (Hofstede Insights, 2022).
"One challenge that confronts humanity, now and in the past, is the degree to which small children are socialized. Without socialization we do not become “human”. This dimension is defined as the extent to which people try to control their desires and impulses, based on the way they were raised. Relatively weak control is called “Indulgence” and relatively strong control is called “Restraint”. Cultures can, therefore, be described as Indulgent or Restrained" (Hofstede Highlights, 2022).
"is the scientific language used by doctors to describe specific medical conditions. Examples of medical terminology could be thrombosis for a blood clot and hypertension for high blood pressure" (Krumrey, 2022).
"is often the shorthand used between people practicing the same profession and it might have no meaning outside the profession. Examples of jargon in the healthcare world would be BP for blood pressure, NPO (nil pers os) or nothing by mouth, and c-section for birth by caesarian section." (Krumrey, 2022).
"According to the biomedical method, doctors look for physical signs of what is wrong. Once the symptom is identified, things like drugs and procedures are used to get rid of the problem. Providers who operate from a biomedical model, might communicate in ways that are efficient and logical. This approach uses relatively little time, and providers might see many patients in a day" (Krumrey, 2022).










 photo: pexel.com[/caption]
photo: pexel.com[/caption]

 I was not just running in and out in 15 minutes. I stayed 3 – THREE – hours with a trusted host. I learned so much. I know you might not take that much time nor find someone to give you such detailed information. I promise you, if you can push yourself to learn more, you can learn to make more complex perceptions. My goal in sharing the following information in this segment is to demonstrate how much I gained from such a short time.
I was not just running in and out in 15 minutes. I stayed 3 – THREE – hours with a trusted host. I learned so much. I know you might not take that much time nor find someone to give you such detailed information. I promise you, if you can push yourself to learn more, you can learn to make more complex perceptions. My goal in sharing the following information in this segment is to demonstrate how much I gained from such a short time. Oh, but there are degrees of HOT or sweet.
Oh, but there are degrees of HOT or sweet. Interpretation = Therefore, I know this is Arbo I will personally buy it for my own salsa preparation.
Interpretation = Therefore, I know this is Arbo I will personally buy it for my own salsa preparation.

 In this week’s discussion, you’ll find an i
In this week’s discussion, you’ll find an i