
4 Module 4: Biological Beginnings
Module 4 Learning Objectives
Upon completion of this module, the learner will be able to:
- Explain Periods of Prenatal Development
Describe the key characteristics and developmental milestones of the germinal, embryonic, and fetal periods, highlighting critical periods of growth, vulnerability to teratogens, and parental influences on development. - Understand Genetic Inheritance
Describe the basic principles of genetic inheritance, including dominant and recessive traits, the role of chromosomes and alleles, and the differences between genotype and phenotype. - Identify Genetic Disorders
Identify common genetic disorders, such as cystic fibrosis and sickle cell anemia, and explain how they are inherited and their impact on development. - Explore Behavioral Genetics
Define behavioral genetics and describe how genetics and environment interact to influence human development and behavior, including gene-environment correlations and epigenetics. - Analyze the Impact of Teratogens
Examine how exposure to teratogens, such as alcohol, tobacco, and environmental chemicals, as well as parental factors, impacts prenatal development and contributes to developmental risks. - Recognize Pregnancy Complications
Describe common complications and side effects of pregnancy, such as preeclampsia and gestational diabetes, and their potential impact on the pregnant person’s comfort, well-being, and the developing fetus. - Explain Labor and Delivery Processes
Explain the signs of labor, the stages of labor, and common interventions used during childbirth, such as cesarean sections and vacuum extractions. - Compare Birthing Practices
Compare and contrast common birthing places and practices, including hospital births, freestanding birth centers, and home births, while analyzing cultural and individual influences on these choices. - Examine Maternal and Infant Mortality
Analyze the role of historical and sociocultural factors in maternal and infant mortality rates, and evaluate strategies to address disparities and improve outcomes. - Understand the APGAR Test
Explain the purpose of the APGAR test, including its scoring system and significance in assessing a newborn’s health immediately after birth. - Differentiate Postpartum Emotional States
Summarize symptoms of postpartum depression and differentiate it from the “baby blues,” including their effects on the parent’s mental health and family dynamics. - Explore Non-Biological Pathways to Parenthood
Describe various ways to make a family outside of childbirth, such as adoption, in vitro fertilization, and foster care, emphasizing their role in expanding definitions of parenthood.
Periods of Prenatal Development
Let’s take a look at some of the changes that take place during each of the three periods of prenatal development: the germinal period, the embryonic period, and the fetal period.
The Germinal Period (Weeks 1-2)

Conception occurs when a sperm fertilizes an egg and forms a zygote, which begins as a one-cell structure. The parents’ DNA is passed on to the child at the moment of conception. The genetic makeup and sex of the baby are set at this point. The germinal period (about 14 days in length) lasts from conception to implantation of the zygote (fertilized egg) in the lining of the uterus.
During the first week after conception, the zygote divides and multiplies, going from a one-cell structure to two cells, then four cells, then eight cells, and so on. The process of cell division is called mitosis. After the fourth division, differentiation of the cells begins to occur as well. Differentiated cells become more specialized, forming different organs and body parts. After 5 days of mitosis, there are 100 cells, and after 9 months there are billions of cells. Mitosis is a fragile process, and fewer than one-half of all zygotes survive beyond the first two weeks (Hall, 2004).
After the zygote divides for about 7–10 days and has 150 cells, it travels down the fallopian tubes and implants itself in the lining of the uterus. It’s estimated that about 60 percent of natural conceptions fail to implant in the uterus. The rate is higher for in vitro conceptions. Once the zygote attaches to the uterus, the next stage begins.
The Embryonic Period (Weeks 3-8)

The embryonic period begins once the zygote is implanted in the uterine wall. It lasts from the third through the eighth week after conception. Upon implantation, this multi-cellular organism is called an embryo. Now blood vessels grow, forming the placenta. The placenta is a structure connected to the uterus that provides nourishment and oxygen from the pregnant person to the developing embryo via the umbilical cord.
During this period, cells continue to differentiate. Basic structures of the embryo start to develop into areas that will become the head, chest, and abdomen. During the embryonic stage, the heart begins to beat and organs form and begin to function. At 22 days after conception, the neural tube forms along the back of the embryo, developing into the spinal cord and brain.
Growth during prenatal development occurs in two major directions: from head to tail (cephalocaudal development) and from the midline outward (proximodistal development). This means that those structures nearest the head develop before those nearest the feet and those structures nearest the torso develop before those away from the center of the body (such as hands and fingers).
The head develops in the fourth week and the precursor to the heart begins to pulse. In the early stages of the embryonic period, gills and a tail are apparent. But by the end of this stage, they disappear and the organism takes on a more human appearance. The embryo is approximately 1 inch in length and weighs about 4 grams at the end of this period. The embryo can move and respond to touch at this time.
About 20 percent of organisms fail during the embryonic period, usually due to gross chromosomal abnormalities. As in the case of the germinal period, often the person does not yet know they are pregnant. It is during this stage that the major structures of the body are taking form making the embryonic period the time when the organism is most vulnerable to the greatest amount of damage if exposed to harmful substances. Potentially pregnant people are not often aware of the risks they introduce to the developing child during this time.
The Fetal Period (Weeks 9-40)

When the organism is about nine weeks old, the embryo is called a fetus. At this stage, the fetus is about the size of a kidney bean and begins to take on the recognizable form of a human being as the “tail” begins to disappear.
From 9–12 weeks, the sex organs begin to differentiate. By the 12th week, the fetus has all its body parts including external genitalia. In the following weeks, the fetus will develop hair, nails, teeth and the excretory and digestive systems will continue to develop. At the end of the 12th week, the fetus is about 3 inches long and weighs about 28 grams.
At about 16 weeks, the fetus is approximately 4.5 inches long. Fingers and toes are fully developed, and fingerprints are visible. During the 4-6th months, the eyes become more sensitive to light and hearing develops. The respiratory system continues to develop. Reflexes such as sucking, swallowing and hiccupping develop during the 5th month. Cycles of sleep and wakefulness are present at that time as well. Throughout the fetal stage, the brain continues to grow and develop, nearly doubling in size from weeks 16 to 28. The majority of the neurons in the brain have developed by 24 weeks although they are still rudimentary and the glial or nerve cells that support neurons continue to grow. At 24 weeks the fetus can feel pain (Royal College of Obstetricians and Gynecologists, 1997).
The first chance of survival outside the womb, known as the age of viability is reached at about 22 to 26 weeks (Moore & Persaud, 1998). By the time the fetus reaches the sixth month of development (24 weeks), it weighs up to 1.4 pounds. The hearing has developed, so the fetus can respond to sounds. The internal organs, such as the lungs, heart, stomach, and intestines, have formed enough that a fetus born prematurely at this point has a chance to survive outside of the uterus.
Between the 7th and 9th months, the fetus is primarily preparing for birth. It is exercising its muscles, its lungs begin to expand and contract. It is developing fat layers under the skin. The fetus gains about 5 pounds and 7 inches during this last trimester of pregnancy which includes a layer of fat gained during the 8th month. This layer of fat serves as insulation and helps the baby regulate body temperature after birth.
Around 36 weeks, the fetus is almost ready for birth. It weighs about 6 pounds and is about 18.5 inches long, and by week 37 all of the fetus’s organ systems are developed enough that it could survive outside the uterus without many of the risks associated with premature birth. The fetus continues to gain weight and grow in length until approximately 40 weeks. By then, the fetus has very little room to move around and birth becomes imminent.

WATCH THIS video below or online for an explanation of the developmental milestones and changes that happen during each month of development for the embryo and fetus. You can view the transcript here .
Genetic Beginnings
Next, we will consider the impact of teratogens. We will also discuss the impact that both parents have on the developing fetus. Then we will present the birth process and some of the complications that can occur during delivery. Before going into these topics, however, it is important to understand how genes and chromosomes affect development.
Heredity
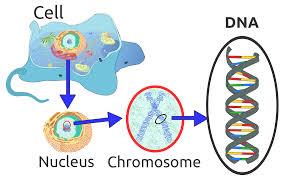
As your recall from earlier reading, nature refers to the contribution of genetics to one’s development. The basic building block of the nature perspective is the gene. Genes are recipes for making proteins, while proteins influence the structure and functions of cells. Genes are located on the chromosomes and there are an estimated 20,500 genes for humans, according to the Human Genome Project (NIH, 2015). See the box below for more details on the Human Genome Project.
The Human Genome Project
In 1990 the Human Genome Project (HGP), an international scientific endeavor, began the task of sequencing the 3 billion base pairs that make up the human genome. In April of 2003, more than two years ahead of schedule, scientists have given us the genetic blueprint for building a human. Since this time, using the information from the HGP, researchers have discovered the genes involved in over 1800 diseases. In 2005 the HGP amassed a large data base called HapMap that catalogs the genetic variations in 11 global populations. Data on genetic variation can improve our understanding of differential risk for disease and reactions to medical treatments, such as drugs. Pharmacogenomic researchers have already developed tests to determine whether a patient will respond favorably to certain drugs used in the treatment of breast cancer or HIV by using information from HapMap (NIH, 2015).
Future directions for the HGP include identifying the genetic markers for all 50 major forms of cancer (The Cancer Genome Atlas), continued use of the HapMap for creating more effective drugs for the treatment of disease, and examining the legal, social and ethical implications of genetic knowledge (NIH, 2015).
From the outset, the HGP made ethical issues one of their main concerns. Part of the HGP’s budget supports research and holds workshops that address these concerns. Who owns this information, and how the availability of genetic information may influence healthcare and its impact on individuals, their families, and the greater community are just some of the many questions being addressed (NIH, 2015).
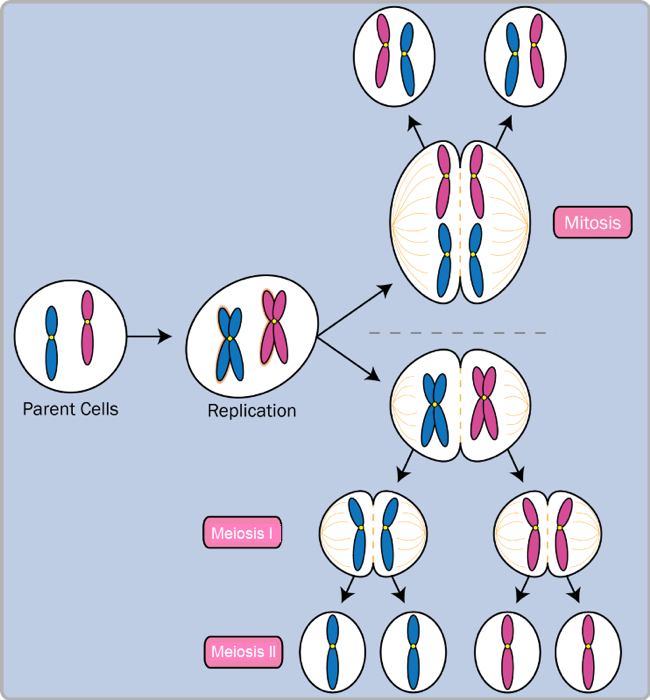
Normal human cells contain 46 chromosomes (or 23 pairs; one from each parent) in the nucleus of the cells. After conception, most cells of the body are created by a process called mitosis.
Mitosis is defined as the cell’s nucleus making an exact copy of all the chromosomes and splitting into two new cells. However, the cells used in sexual reproduction, called the gametes (sperm or ova), are formed in a process called meiosis. In meiosis the gamete’s chromosomes duplicate, and then divide twice resulting in four cells containing only half the genetic material of the original gamete. Thus, each sperm and egg possess only 23 chromosomes and combine to produce the normal 46. Given the amount of genes present and the unpredictability of the meiosis process, the likelihood of having offspring that are genetically identical (and not twins) is one in trillions (Gould & Keeton, 1997).
Of the 23 pairs of chromosomes created at conception, 22 pairs are similar in length. These are called autosomes. The remaining pair, or sex chromosomes, may differ in length. If a child receives the combination of XY the child will be genetically male. If the child receives the combination XX the child will be genetically female. Many genetic variations can occur within the sex chromosomes. For instance, people who have Turner syndrome typically have only one sex chromosome, an X, and people with Klinefelter syndrome have an extra X chromosome (XXY).
Genetic variations and inheritance
Genetic variation, the genetic differences between individuals, is what contributes to a species’ ability to adapt to its environment. In humans, genetic variation begins with an egg, several million sperm, and fertilization. The egg and the sperm each contain 23 chromosomes, which make up our genes. A single gene may have multiple possible variations or alleles (a specific version of a gene), resulting in a variety of combinations of inherited traits.
Genetic inheritance of traits for humans is based upon Gregor Mendel’s model of inheritance. For genes on an autosome (any chromosome other than a sex chromosome), the alleles and their associated traits are autosomal dominant or autosomal recessive. In this model, some genes are considered dominant because they will be expressed. Others, termed recessive, are only expressed in the absence of a dominant gene. Some characteristics that were once thought of as dominant-recessive, such as eye color, are now believed to be a result of the interaction between several genes. Dominant traits include curly hair, facial dimples, normal vision, and dark hair. Recessive characteristics include red hair, pattern baldness, and nearsightedness.
Sickle cell anemia is an autosomal recessive disease; Huntington disease is an autosomal dominant disease. Other traits are a result of partial dominance or co-dominance in which both genes are influential. For example, if a person inherits both recessive genes for cystic fibrosis, the disease will occur. But if a person has only one recessive gene for the disease, the person would be a carrier of the disease.
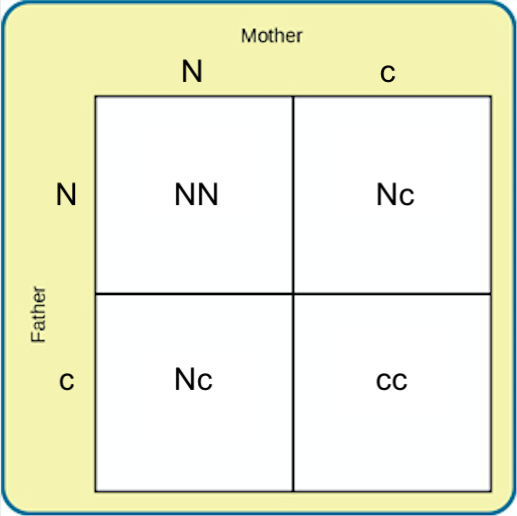
In this example, we will call the normal gene “N,” and the gene for cystic fibrosis “c.” The normal gene is dominant, which means that having the dominant allele either from one parent (Nc) or both parents (NN) will always result in the phenotype associated with the dominant allele. When someone has two copies of the same allele, they are said to be homozygous for that allele. When someone has a combination of alleles for a given gene, they are said to be heterozygous. For example, cystic fibrosis is a recessive disease which means that an individual will only have the disease if they are homozygous for that recessive allele (cc).
Imagine that a woman who is a carrier of the cystic fibrosis gene has a child with a man who also is a carrier of the same disease. What are the odds that their child would inherit the disease? Both the woman and the man are heterozygous for this gene (Nc). We can expect the offspring to have a 25% chance of having cystic fibrosis (cc), a 50% chance of being a carrier of the disease (Nc), and a 25% chance of receiving two normal copies of the gene (NN).
Gene mutations are one source of harmful genes. A mutation is a sudden, permanent change in a gene. While many mutations can be harmful or lethal, some mutations are beneficial by giving a person an advantage over those who do not have the mutation. Recall that the theory of evolution maintains that individuals best adapted to their particular environments are more likely to reproduce and pass on their genes to future generations. In order for this process to occur, there must be variability in genes (and resultant traits) that allow for variation in adaptability to the environment. If a population consisted of identical individuals, then any dramatic changes in the environment would affect everyone in the same way, and there would be no variation in selection. In contrast, diversity in genes and associated traits allows some individuals to perform slightly better than others when faced with environmental change. This creates a distinct advantage for individuals best suited for their environments in terms of successful reproduction and genetic transmission.
Genotypes and Phenotypes
The word genotype refers to the sum total of all the genes a person inherits. The word phenotype refers to the features that are actually expressed. Look in the mirror. What do you see, your genotype or your phenotype? What determines whether or not genes are expressed? Because genes are inherited in pairs on the chromosomes, we may receive either the same version of a gene from both parents, that is, be homozygous for that characteristic the gene influences. If we receive a different version of the gene from each parent, that is referred to as heterozygous. In the homozygous situation we will display that characteristic. It is in the heterozygous condition that it becomes clear that not all genes are created equal. Some genes are dominant, meaning they express themselves in the phenotype even when paired with a different version of the gene, while their silent partner is called recessive. Recessive genes express themselves only when paired with a similar version gene.
Geneticists refer to different versions of a gene as alleles. Some dominant traits include having facial dimples, curly hair, normal vision, and dark hair. Some recessive traits include red hair, being nearsighted, and straight hair.
Most characteristics are not the result of a single gene; they are polygenic, meaning they are the result of several genes. In addition, the dominant and recessive patterns described above are usually not that simple either. Sometimes the dominant gene does not completely suppress the recessive gene; this is called incomplete dominance. An example of this can be found in the recessive gene disorder sickle cell disease. The gene that produces healthy round-shaped red blood cells is dominant. The recessive gene causes an abnormality in the shape of red blood cells; they take on a sickle form, which can clog the veins and deprive vital organs of oxygen and increase the risk of stroke. To inherit the disorder a person must receive the recessive gene from both parents. Those who have inherited only one recessive-gene are called carriers and should be unaffected by this recessive trait. Yet, carriers of sickle cell have some red blood cells that take on the c-shaped sickle pattern. Under circumstances of oxygen deprivation, such as high altitudes or physical exertion, carriers for the sickle cell gene may experience some of the symptoms of sickle cell.
Monozygotic and Dizygotic Twins
Many students are interested in twins. Monozygotic or identical twins occur when a fertilized egg splits apart in the first two weeks of development. The result is the creation of two separate, but genetically identical offspring. That is, they possess the same genotype and often the same phenotype.

About one-third of twins are monozygotic twins. Sometimes, however, two eggs or ova are released and fertilized by two separate sperm. The result is dizygotic or fraternal twins. These two individuals share the same amount of genetic material as would any two children from the same parents. In other words, they possess a different genotype and phenotype. Pregnancies resulting from older eggs are more likely to have dizygotic twins as are pregnancies where fertility drugs are used. There has been an increase in the number of fraternal twins recently.

Twin Studies
Research comparing monozygotic and dizygotic twins, and often also comparing twins who were raised in biological parental versus adoptive parental households, can tell us a lot about genetic influences. These research studies are called “twin studies.”
Using the variables of height and spoken language, let’s take a look at how nature and nurture apply: Identical twins, unsurprisingly, are almost perfectly similar for height. The heights of fraternal twins, however, are like any other sibling pairs: more similar to each other than to people from other families, but hardly identical. This contrast between twin types gives us a clue about the role genetics plays in determining height. Now consider spoken language. If one identical twin speaks Spanish at home, the co-twin with whom she is raised almost certainly does too. But the same would be true for a pair of fraternal twins raised together. In terms of spoken language, fraternal twins are just as similar as identical twins, so it appears that the genetic match of identical twins doesn’t make much difference.
Twin and adoption studies are two instances of a much broader class of methods for observing nature-nurture called quantitative genetics, the scientific discipline in which similarities among individuals are analyzed based on how biologically related they are. We can do these studies with siblings and half-siblings, cousins, twins who have been separated at birth and raised separately (Bouchard, Lykken, McGue, & Segal, 1990; such twins are very rare and play a smaller role than is commonly believed in the science of nature–nurture), or with entire extended families.
It would be satisfying to be able to say that nature–nurture studies have given us conclusive and complete evidence about where traits come from, with some traits clearly resulting from genetics and others almost entirely from environmental factors, such as childrearing practices and personal will; but that is not the case. Instead, everything has turned out to have some footing in genetics. The more genetically-related people are, the more similar they are—for everything: height, weight, intelligence, personality, mental illness, etc. Sure, it seems like common sense that some traits have a genetic bias. For example, adopted children resemble their biological parents even if they have never met them, and identical twins are more similar to each other than are fraternal twins. And while certain psychological traits, such as personality or mental illness (e.g., schizophrenia), seem reasonably influenced by genetics, it turns out that the same is true for political attitudes, how much television people watch (Plomin, Corley, DeFries, & Fulker, 1990), and whether or not they get divorced (McGue & Lykken, 1992). You can’t leave genes out of the equation. But keep in mind, no behavioral traits are completely inherited, so you can’t leave the environment out altogether, either.
LISTEN TO THIS Learn more by listening to the podcast “What studying twins can teach us about ourselves,” part of the Speaking of Psychology series by the American Psychological Association. Listen with captions here.
READ THIS For more information on how genetics and environment intertwine in development, read the article Gene-Environment-Interaction by the Center on the Developing Child at Harvard University.
Genetic Disorders
Most of the known genetic disorders are dominant gene-linked; however, the vast majority of dominant gene linked disorders are not serious or debilitating. For example, the majority of those with Tourette’s Syndrome suffer only minor tics from time to time and can easily control their symptoms. Huntington’s Disease is a dominant gene linked disorder that affects the nervous system and is fatal, but does not appear until midlife. Recessive gene disorders, such as cystic fibrosis and sickle-cell anemia, are less common but may actually claim more lives because they are less likely to be detected as people are unaware that they are carriers of the disease. Some genetic disorders are sex-linked; the defective gene is found on the X-chromosome. Males have only one X chromosome so are at greater risk for sex-linked disorders due to a recessive gene, such as hemophilia, color-blindness, and baldness. For females to be affected by the genetic defects, they need to inherit the recessive gene on both X-chromosomes, but if the defective gene is dominant, females can be equally at risk. The following table lists several genetic disorders.
Table of Genetic Disorders
Recessive Disorders (Homozygous): The individual inherits a gene change from both parents. If the gene is inherited from just one parent, the person is a carrier and does not have the condition. |
Cases per Birth |
|
Sickle Cell Disease (SCD) is a condition in which the red blood cells in the body are shaped like a sickle (like the letter C) and affect the ability of the blood to transport oxygen. Carriers may experience some effects, but do not have the full condition. |
1 in 500 Black births 1 in 36,000 Hispanic births |
|
Cystic Fibrosis (CF) is a condition that affects breathing and digestion due to thick mucus building up in the body, especially the lungs and digestive system. In CF, the mucus is thicker than normal and sticky. |
1 in 3500 |
|
Phenylketonuria (PKU) is a metabolic disorder in which the individual cannot metabolize phenylalanine, an amino acid. Left untreated intellectual deficits occur. PKU is easily detected and is treated with a special diet. |
1 in 10,000 |
|
Tay Sachs Disease is caused by enzyme deficiency resulting in the accumulation of lipids in the nerve cells of the brain. This accumulation results in progressive damage to the cells and a decrease in cognitive and physical development. Death typically occurs by age five. |
1 in 4000 1in 30 American Jews is a carrier 1 in 20 French Canadians is a carrier |
|
Albinism is when the individual lacks melanin and possesses little to no pigment in the skin, hair, and eyes. Vision problems can also occur. |
Fewer than 20,000 US cases per year |
|
|
|
Autosomal Dominant Disorders (Heterozygous): In order to have the disorder, the individual only needs to inherit the gene change from one parent. |
Cases per Birth |
|
Huntington’s Disease is a condition that affects the individual’s nervous system. Nerve cells become damaged, causing various parts of the brain to deteriorate. The disease affects movement, behavior and cognition. It is fatal, and occurs at midlife. |
1 in 10,000 |
|
Tourette Syndrome is a tic disorder which results in uncontrollable motor and vocal tics as well as body jerking. |
1 in 250 |
|
Achondroplasia is the most common form of disproportionate short stature. The individual has abnormal bone growth resulting in short stature, disproportionately short arms and legs, short fingers, a large head, and specific facial features. |
1 in 15,000-40,000 |
|
|
|
Sex-Linked Disorders: When the X chromosome carries the mutated gene, the disorder is referred to as an X-linked disorder. Males are more affected than females because they possess only one X chromosome without an additional X chromosome to counter the harmful gene. |
Cases per Birth |
|
Fragile X Syndrome occurs when the body cannot make enough of a protein it needs for the brain to grow and problems with learning and behavior can occur. Fragile X syndrome is caused from an abnormality in the X chromosome, which then breaks. If a female has fragile X, her second X chromosome usually is healthy, but males with fragile X don’t have a second healthy X chromosome. This is why symptoms of fragile X syndrome usually are more serious in males. |
1 in 4000 males 1 in 8000 females |
|
Hemophilia occurs when there are problems in blood clotting causing both internal and external bleeding. |
1 in 10,000 males |
|
Duchenne Muscular Dystrophy is a weakening of the muscles resulting in an inability to move, wasting away, and possible death. |
1 in 3500 males |
Chromosomal Abnormalities
A chromosomal abnormality occurs when a child inherits too many or too few chromosomes. The most common cause of chromosomal abnormalities is the age of the pregnant person. A 20-year-old pregnant person has a 1 in 800 chance of having a child with a common chromosomal abnormality. A 44-year-old pregnant person, however, has a one in 16 chance. It is believed that the problem occurs when the ovum is ripening prior to ovulation each month. As the pregnant person ages, the ovum is more likely to suffer abnormalities at this time.
Another common cause of chromosomal abnormalities occurs because the gametes do not divide evenly when they are forming. Therefore, some cells have more than 46 chromosomes. In fact, it is believed that close to half of all zygotes have an odd number of chromosomes. Most of these zygotes fail to develop and are spontaneously aborted by the body. If the abnormal number occurs on pair # 21 or # 23, however, the individual may have certain physical or other abnormalities. See the table below for additional information.
One of the most common chromosomal abnormalities is on pair # 21. Trisomy 21 occurs when there are three rather than two chromosomes on #21. A person with Down syndrome has distinct facial features, intellectual variations, and oftentimes heart and gastrointestinal disorders. Symptoms vary from person to person and can range from mild to severe. With early intervention, the life expectancy of persons with Down syndrome has increased in recent years. Keep in mind that there is as much variation in people with Down syndrome as in most populations and those differences need to be recognized and appreciated.
WATCH THIS To learn more, watch the video clip below or online with captions about Down syndrome from the National Down Syndrome Society. You can view the transcript for “Down syndrome – Ability Awareness PSA Video” here.
Table of Chromosomal Disorders |
|
Autosomal Chromosome Disorders: The individual inherits too many or two few chromosomes. |
Cases per Birth |
|
Down syndrome/Trisomy 21 is caused by an extra chromosome 21 and includes a combination of birth defects. Affected individuals have some degree of intellectual variations, characteristic facial features, often heart defects, and other health problems. The severity varies greatly among affected individuals. |
1 in 691 1 in 300 births at age 35 |
|
Trisomy 13 is caused by an extra chromosome 13. Affected individuals have multiple birth defects and generally die in the first weeks or months of life. |
1 in 7,906 |
|
Trisomy 18 is caused by an extra chromosome 18 and the affected individual also has multiple birth defects within many areas of the body and typically results in early death. |
1 in 3,762 |
Sex-Linked Chromosomal Disorders: The disorder occurs on chromosome pair #23 or the sex chromosomes. |
Cases per Birth |
|
Turner Syndrome is caused when all or part of one of the X chromosomes is lost before or soon after conception due to a random event. The resulting zygote has an XO composition. Turner Syndrome typically affects cognitive functioning and sexual maturation in girls. Infertility and a short stature may be noted. |
1 in 2500 females |
|
Klinefelter Syndrome is caused when an extra X chromosome is present in the cells of a male due to a random event. The Y chromosome stimulates the growth of male genitalia, but the additional X chromosome inhibits this development. The male may have some breast development, infertility, and low levels of testosterone. |
1 in 700 males |
Genetic Counseling
Genetic counseling refers to a service that assists individuals identify, test for, and explain potential genetic conditions that could adversely affect themselves or their offspring (CDC, 2015b). The common reasons for genetic counseling include:
Family history of a genetic condition
Membership in a certain ethnic group with a higher risk of a genetic condition
Information regarding the results of genetic testing, including blood tests, amniocentesis, or ultra sounds
Learning about the chances of having a baby with a genetic condition if the person is older, has had several miscarriages, has offspring with birth defects, experiences infertility, or has a medical condition
Behavioral Genetics
Behavioral Genetics is the scientific study of the interplay between the genetic and environmental contributions to behavior. Often referred to as the nature/nurture debate, Gottlieb (1998, 2000, 2002) suggests an analytic framework for this debate that recognizes the interplay between the environment, behavior, and genetic expression. This bidirectional interplay suggests that the environment can affect the expression of genes just as genetic predispositions can impact a person’s potentials. Additionally, environmental circumstances can trigger symptoms of a genetic disorder. For example, a person who has sickle cell anemia, a recessive gene linked disorder, can experience a sickle cell crisis under conditions of oxygen deprivation. Someone predisposed genetically for type-two diabetes can trigger the disease through poor diet and little exercise.
Research has shown how the environment and genotype interact in several ways. Genotype- Environment Correlations refer to the processes by which genetic factors contribute to variations in the environment (Plomin, DeFries, Knopik, & Niederhiser, 2013). There are three types of genotype-environment correlations:
Passive genotype-environment correlation occurs when children passively inherit the genes and the environments their family provides. Certain behavioral characteristics, such as being athletically inclined, may run in families. The children have inherited both the genes that would enable success at these activities, and given the environmental encouragement to engage in these actions. Figure 2.3 highlights this correlation by demonstrating how a family passes on water skiing skills through both genetics and environmental opportunities.
Evocative genotype-environment correlation refers to how the social environment reacts to individuals based on their inherited characteristics. For example, whether one has a more outgoing or shy temperament will affect how he or she is treated by others.
Active genotype-environment correlation occurs when individuals seek out environments that support their genetic tendencies. This is also referred to as niche picking. For example, children who are musically inclined seek out music instruction and opportunities that facilitate their natural musical ability.
Conversely, Genotype-Environment Interactions involve genetic susceptibility to the environment. Adoption studies provide evidence for genotype-environment interactions. For example, the Early Growth and Development Study (Leve, Neiderhiser, Scaramella, & Reiss, 2010) followed 360 adopted children and their adopted and biological parents in a longitudinal study. Results have shown that children whose biological parents exhibited psychopathology, exhibited significantly fewer behavior problems when their adoptive parents used more structured parenting than unstructured. Additionally, elevated psychopathology in adoptive parents increased the risk for the children’s development of behavior problems, but only when the biological parents’ psychopathology was high. Consequently, the results show how environmental effects on behavior differ based on the genotype, especially stressful environments on genetically at-risk children.
Lastly, Epigenetics studies modifications in DNA that affect gene expression and are passed on when the cells divide. Environmental factors, such as nutrition, stress, and teratogens are thought to change gene expression by switching genes on and off. These gene changes can then be inherited by daughter cells. This would explain why monozygotic or identical twins may increasingly differ in gene expression with age. For example, Fraga et al. (2005) found that when examining differences in DNA, a group of monozygotic twins were indistinguishable during the early years. However, when the twins were older there were significant discrepancies in their gene expression, most likely due to different experiences. These differences included susceptibilities to disease and a range of personal characteristics.
Teratology
Good prenatal care is essential. The developing child is most at risk for some of the most severe problems during the first three months of development. Unfortunately, this is a time at which most people are unaware that they are pregnant. It is estimated that 10% of all birth defects are caused by a prenatal exposure or teratogen. Teratogens are factors that can contribute to birth defects which include some maternal diseases, drugs, alcohol, and stress. These exposures can also include environmental and occupational exposures. Today, we know many of the factors that can jeopardize the health of the developing child. Teratogen-caused birth defects are potentially preventable.
The study of factors that contribute to birth defects is called teratology. Teratogens are usually discovered after an increased prevalence of a particular birth defect. For example, in the early 1960’s, a drug known as thalidomide was used to treat morning sickness. Exposure of the fetus during this early stage of development resulted in cases of phocomelia, a congenital malformation in which the hands and feet are attached to abbreviated arms and legs.
A Look at Some Teratogens
Alcohol
One of the most commonly used teratogens is alcohol. Because half of all pregnancies in the United States are unplanned, it is recommended that women of child-bearing age take great caution against drinking alcohol when not using birth control and when pregnant (Surgeon General’s Advisory on Alcohol Use During Pregnancy, 2005). Alcohol consumption, particularly during the second month of prenatal development, but at any point during pregnancy, may lead to neurocognitive and behavioral difficulties that can last a lifetime.
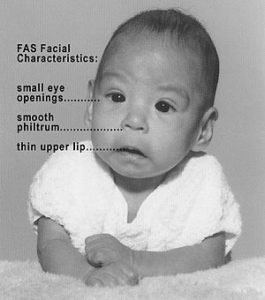
There is no acceptable safe limit for alcohol use during pregnancy, but binge drinking (5 or more drinks on a single occasion) or having 7 or more drinks during a single week places a child at particularly high risk. In extreme cases, alcohol consumption can lead to fetal death, but more frequently it can result in fetal alcohol spectrum disorders (FASD). This terminology is now used when looking at the effects of exposure and replaces the term fetal alcohol syndrome. It is preferred because it recognizes that symptoms occur on a spectrum and that all individuals do not have the same characteristics. Children with FASD share certain physical features such as flattened noses, small eye openings, small heads, intellectual developmental delays, and behavioral problems. Those with FASD are more at risk for lifelong problems such as criminal behavior, psychiatric problems, and unemployment (CDC, 2006).
The terms alcohol-related neurological disorder (ARND) and alcohol-related birth defects (ARBD) have replaced the term Fetal Alcohol Effects to refer to those with less extreme symptoms of FASD. ARBD include kidney, bone and heart problems.
WATCH THIS video below or online with captions where several medical experts debunk common myths about the safety of drinking alcohol during pregnancy. You can view the transcript for “NOFAS Topics: Light Drinking” here.
Tobacco
Smoking is also considered a teratogen because nicotine travels through the placenta to the fetus. When the pregnant person smokes, the developing baby experiences a reduction in blood oxygen levels. Tobacco use during pregnancy has been associated with low birth weight, placenta previa, birth defects, preterm delivery, fetal growth restriction, and sudden infant death syndrome. Smoking in the month before getting pregnant and throughout pregnancy increases the chances of these risks. Quitting smoking before getting pregnant is best. However, for people who are already pregnant, quitting as early as possible can still help protect against some health problems for both them and the developing pregnancy.
Drugs
Prescription, over-the-counter, or recreational drugs can have serious teratogenic effects. In general, if medication is required, the lowest dose possible should be used. Combination drug therapies and first trimester exposures should be avoided. Almost three percent of pregnant women use illicit drugs such as marijuana, cocaine, Ecstasy and other amphetamines, and heroin. These drugs can cause low birth-weight, withdrawal symptoms, birth defects, or learning or behavioral problems. Babies born with a heroin addiction need heroin just like an adult addict. The child will need to be gradually weaned from the heroin under medical supervision; otherwise, the child could have seizures and die.
Environmental Chemicals
Environmental chemicals can include an exposure to a wide array of agents including pollution, organic mercury compounds, herbicides, and industrial solvents. Some environmental pollutants of major concern include lead poisoning, which is connected with low birth weight and slowed neurological development. Children who live in older housing in which lead-based paints have been used have been known to eat peeling paint chips thus being exposed to lead. The chemicals in certain herbicides are also potentially damaging. Radiation is another environmental hazard that a pregnant woman must be aware of. If a pregnant person is exposed to radiation, particularly during the first three months of pregnancy, the child may suffer some congenital deformities. There is also an increased risk of miscarriage and stillbirth. Mercury leads to physical deformities and intellectual disabilities (Dietrich, 1999).
Sexually Transmitted Infections
Sexually transmitted infections (STIs) can complicate pregnancy and may have serious effects on both the pregnant person and the developing baby. Most prenatal care today includes testing for STIs, and early detection is important. STIs, such as chlamydia, gonorrhea, syphilis, trichomoniasis and bacterial vaginosis can all be treated and cured with antibiotics that are safe to take during pregnancy. STIs that are caused by viruses, like genital herpes, hepatitis B, or HIV cannot be cured. However, in some cases these infections can be treated with antiviral medications or other preventive measures can be taken to reduce the risk of passing the infection to the baby.
Maternal Diseases
Maternal illnesses increase the chance that a baby will be born with a birth defect or have a chronic health problem. Some of the diseases that are known to potentially have an adverse effect on the fetus include: diabetes, cytomegalovirus, toxoplasmosis, Rubella, varicella, hypothyroidism, and Strep B. If the pregnant person contracts Rubella during the first three months of pregnancy, damage can occur in the eyes, ears, heart, or brain of the unborn child. On a positive note, Rubella has been nearly eliminated in the industrial world due to the vaccine created in 1969. Diagnosing these diseases early and receiving appropriate medical care can help improve the outcomes. Routine prenatal care now includes screening for gestational diabetes and Strep B.
Maternal Stress
Stress represents the effects of any factor able to threaten the homeostasis of an organism; these either real or perceived threats are referred to as the “stressors” and comprise a long list of potentially adverse factors, which can be emotional or physical. Because of a link in blood supply between the pregnant person and fetus, it has been found that stress can leave lasting effects on a developing fetus, even before a child is born. The best-studied outcomes of fetal exposure to maternal prenatal stress are preterm birth and low birth weight. Maternal prenatal stress is also considered responsible for a variety of changes of the child’s brain, and a risk factor for conditions such as behavioral problems, learning disorders, high levels of anxiety, attention deficit hyperactivity disorder, autism, and schizophrenia. Furthermore, maternal prenatal stress has been associated with a higher risk for a variety of immune and metabolic changes in the child such as asthma, allergic disorders, cardiovascular diseases, hypertension, hyperlipidemia, diabetes, and obesity.
Paternal Impact
Most teratogens focus on the pregnant person and exposure of the ovum or uterus, but there are also teratogenic effects to sperm.
READ THIS: For some common teratogens and research about how they affect a pregnancy, read the Paternal Exposures fact sheet.
Below are just a few paternal exposure factors.
The age of fathers at the time of conception is also an important factor in health risks for children. According to Nippoldt (2015) offspring of men over 40 face an increased risk of miscarriages, autism, congenital disabilities, achondroplasia (bone growth disorder), and schizophrenia. These increased health risks are thought to be due to accumulated chromosomal aberrations and mutations during the maturation of sperm cells in older men (Bray, Gunnell, & Smith, 2006). However, like older women, the overall risks are small.
Also, men are more likely than women to work in occupations where hazardous chemicals, many of which have teratogenic effects or may cause genetic mutations, are used (Cordier, 2008). These may include petrochemicals, lead, and pesticides that can cause abnormal sperm and lead to miscarriages or diseases. Men are also more likely to be a source of second-hand smoke for their developing offspring. Smoking around the pregnant person can hinder fetal development.
Factors influencing prenatal risks
There are several considerations in determining the type and amount of damage that might result from exposure to a particular teratogen (Berger, 2004). These include:
The timing of the exposure: Structures in the body are vulnerable to the most severe damage when they are forming. If a substance is introduced during a particular structure’s critical period (time of development), the damage to that structure may be greater. For example, the ears and arms reach their critical periods at about 6 weeks after conception. If a pregnant person exposes the embryo to certain substances during this period, the arms and ears may be malformed.
The amount of exposure: Some substances are not harmful unless the amounts reach a certain level. The critical level depends in part on the size and metabolism of the pregnant person.
Genetics: Genetic make-up also plays a role on the impact a particular teratogen might have on the child. This is suggested by fraternal twin studies who are exposed to the same prenatal environment, yet do not experience the same teratogenic effects. The genetic make-up of the pregnant person can also have an effect; some may be more resistant to teratogenic effects than others.
Sex chromosomes: Genetically males are more likely to experience damage due to teratogens than are females. It is believed that the Y chromosome, which contains fewer genes than the X, may have an impact.
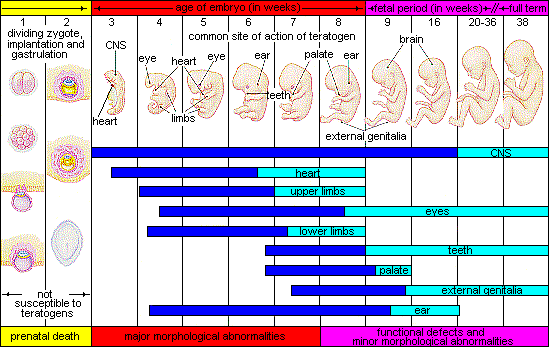
Critical Periods of Prenatal Development. The above image summarizes the three developmental periods in prenatal development. The blue images indicate where major development is happening and the aqua indicate where refinement is happening. As shown, the majority of organs are particularly susceptible during the embryonic period. The central nervous system still continues to develop in major ways through the fetal period as well.
Complications of Pregnancy
Minor complications: There are a number of common side effects of pregnancy. Not everyone experiences all of these nor to the same degree. And although they are considered “minor” this is not to say that these problems are potentially very uncomfortable. These side effects include nausea (particularly during the first 3-4 months of pregnancy as a result of higher levels of estrogen in the system), heartburn, gas, hemorrhoids, backache, leg cramps, insomnia, constipation, shortness of breath or varicose veins (as a result of carrying a heavy load on the abdomen). What is the cure? Delivery!
Major Complications: The following are some serious complications of pregnancy which can pose health risks to pregnant person and child and that often require special care.
- Ectopic pregnancy occurs when the zygote becomes attached to the fallopian tube before reaching the uterus. About 1 in 50 pregnancies in the United States are tubal pregnancies and this number has been increasing because of the higher rates of pelvic inflammatory disease and Chlamydia (Carroll, 2007). Abdominal pain, vaginal bleeding, nausea and fainting are symptoms of ectopic pregnancy.
- Toxemia or blood poisoning due to kidney malfunction is experienced by 6 to 7 percent of women during their last months of pregnancy. If untreated toxemia can lead to preeclampsia or swelling and hypertension or progress to eclampsia which is can involve coma or death.
- Gestational diabetes is when a woman without diabetes develops high blood sugar levels during pregnancy.
Hyperemesis gravidarum is the presence of severe and persistent vomiting, causing dehydration and weight loss. It is more severe than the more common morning sickness.
Preeclampsia or gestational hypertension. Severe preeclampsia involves blood pressure over 160/110 with additional signs. Eclampsia is seizures in a patient who is pre-eclamptic.
Deep vein thrombosis is the formation of a blood clot in a deep vein, most commonly in the legs.
A pregnant woman is more susceptible to infections. This increased risk is caused by an increased immune tolerance in pregnancy to prevent an immune reaction against the fetus.
Peripartum cardiomyopathy is a decrease in heart function which occurs in the last month of pregnancy, or up to six months post-pregnancy.
Childbirth
Pre-Labor Signs: as your body is preparing for labor, there are a few things that should be expected to happen within four to six weeks of labor.
- Pressure on the pelvic area
- Occasional brownish discharge
- Energy level is noticeably increasing or decreasing
- Loss of the mucus plug (does not always exist)/increasing discharge
- Braxton Hicks contractions (painless contraction of the uterus)
- Movement of the baby into the pelvis
False Labor Signs: there are a few signs that indicate false labor.
- Timing of the contractions are irregular and do not become more frequent or more intense
- Contractions stop during rest, stopping what the mother is doing, walking, or changing position
- Inconsistent in strength (strong one minute then weak the next)
- Location of pain is in the front only
True Labor
- Pain in the lower back, radiating towards the front abdomen, possibly also the legs
- Contractions increase in strength and are closer together; coming now on a regular basis, 30 to 70 seconds apart
- The mucous plug is detached, showing bloody discharge
- The water breaks (often this does not break until the doctor or nurse midwife does it), when this happens, contractions become much stronger
- Some women have the sudden need to go to the bathroom, diarrhea is common
- Contractions continue despite movement
- The cervix is thinning and dilating
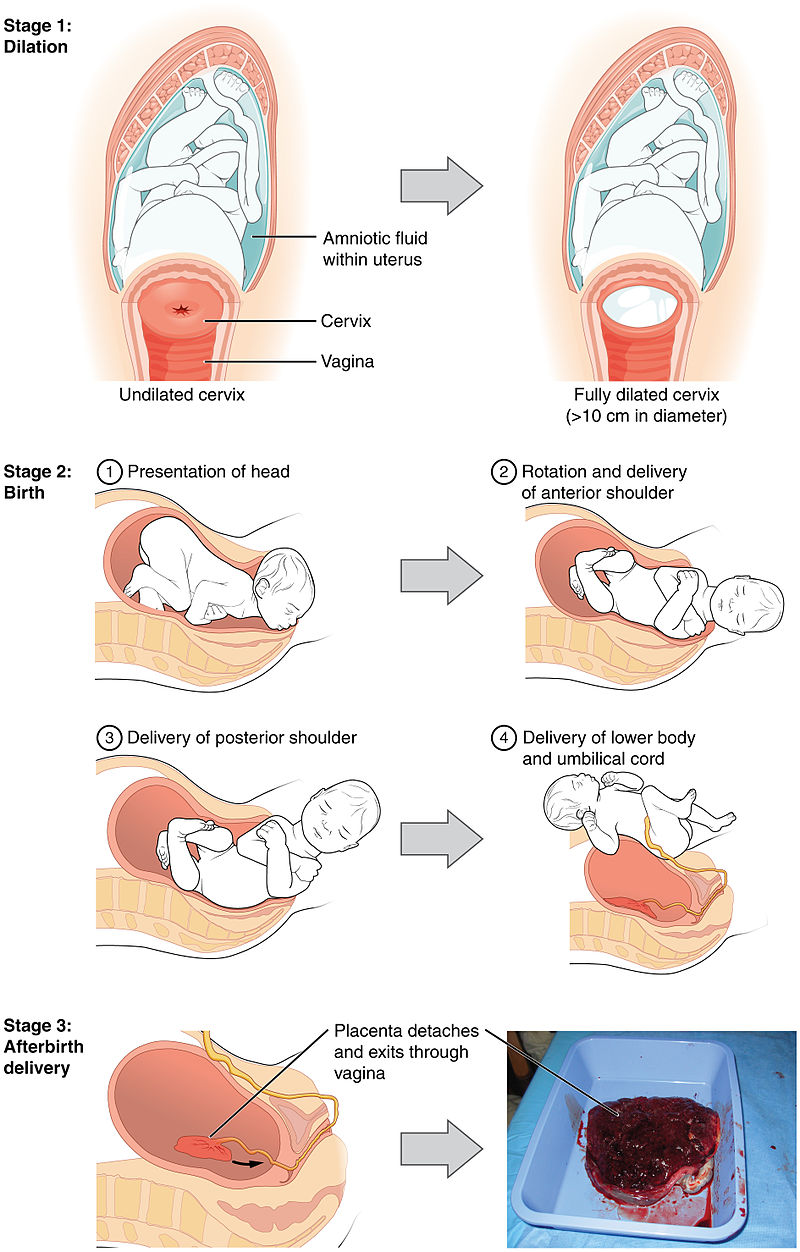
When the contractions of labor begin, the walls of the uterus start to contract. They are stimulated by the release of the pituitary hormone oxytocin. The contractions cause the cervix to dilate (open) and efface (thin out) . As labor progresses the amniotic sac can rupture causing a slow or a fast gush of fluids. Labor usually begins within a 24 hour period after the amniotic sac has ruptured. As contractions become closer and stronger the cervix will gradually start to dilate. The first stage of labor is broken into three parts:
Early Phase: First is the early phase of labor, when the cervix dilates from 1-4 centimeters, this can be the longest and most exhausting part for the mother.
Active Phase: The cervix dilates on average 1 cm per hour in the active phase of labor dilating from 4-7 centimeters. If an epidural is requested, it is usually given in this phase.
Transition: This is often considered the most intense part of labor with contractions lasting longer and having shorter rest periods in between them. Dilation from 8-10 centimeters occurs during transition. Some women experience nausea and vomiting during this phase as well as rectal pressure and an urge to push.
At this point the labor enters the second stage, or the birth of the baby. The mother begins pushing to aid in the birth of the baby, this part of labor can last minutes, or even hours. A fetus is usually delivered head first. ‘Crowning’ is the term used when the fetus’ head can be seen between the mothers labia as it emerges. At this point, the birth attendant may perform an episiotomy if necessary, which is a small surgical incision on the perineum. This procedure is usually done to deliver the baby more quickly, in response to fetal distress.
The third stage of labor is the delivery of the afterbirth (placenta). Oxytocin continues to be released to shrink the size of the uterus and aid in the limiting of blood loss from the site of the placenta. As the uterus shrinks the attachment site blood vessels, some of which can be as large as an adult finger, shrink also. The average blood loss in a routine vaginal delivery is 400-500 cc.
There are times when a mother may need outside aid in the delivery of the baby, some of these methods include:
Forceps, an instrument used to cradle the fetus’ head and manipulate the head under the pubic bone to more easily pass through the birth canal.
Vacuum Extraction, a suction cup is applied to the baby’s head, and a plunger is used to suck any air from between the suction cup and the head to create a good seal. The baby’s head is then manipulated through the birth canal. This usually leaves a baby’s head bruised, but the mark fades within weeks after birth.
Cesarean section, also known as C-section, is the delivery of a baby through a surgical abdominal incision (Abdominal delivery – Abdominal birth – Cesarean section). A C-section delivery is performed when a vaginal birth is not possible or is not safe for the mother or child. Surgery is usually done while the woman is awake but anesthetized from the chest to the legs by epidural or spinal anesthesia. An incision is made across the abdomen just above the pubic area. The uterus is opened, and often brought through the incision after delivery for better visualization. The amniotic fluid is drained, and the baby is delivered. The baby’s mouth and nose are cleared of fluids, and the umbilical cord is clamped and cut. After delivery, a Newborn Intensive Care Unit (NICU) nurse, nurse midwife, nurse practitioner, neonatologist or pediatrician checks to make sure that the baby is breathing and responding. Due to a variety of medical and social factors, C-sections have become fairly common; around 25% of births are performed by C-section. C-sections carry some risks to mother and baby. Compared to a vaginal birth, the risks to mother include increased risk of death, surgical injury, infection, postpartum depression, and hemorrhage, although these are rare. Babies born by c-section are more likely to be admitted to the NICU for breathing problems.

Delivery Options
Hospital Births
The chances of having a natural, uncomplicated birth are optimized by carefully selecting your obstetrician and hospital. Doctors who work with midwives have lower Cesarean section rates because midwives handle less complicated pregnancies. Delivering babies by abdominal surgery has been steadily rising in America over the past two decades, so that now 22-30% of births in American hospitals are by Cesarean section. The U.S., despite having the most advanced technology and highly trained medical personnel, ranks 23rd in infant mortality and 18th in perinatal mortality.
Medical interventions such as epidural anesthesia, pitocin augmentation of labor, vacuum extraction of the fetus, episiotomy and separation of newborn and mother are common in American hospitals. There are circumstances where medical procedures such as these are necessary, but many parents and professionals now question the routine use of such interventions. In some cases, the routine use of these procedures have led to further complications. For example, the epidural anesthetic, while providing pain relief, has shown to increase the operative vaginal delivery rate (i.e. forceps and vacuum extraction rates slightly), especially in first time mothers. Epidurals have not been shown to increase the cesarean section rate in recent well documented studies.
Freestanding Birth Centers & Water Birth
“Freestanding” Birth Centers are not inside of or affiliated with a hospital. They are run by a collaboration of midwives and/or physicians. This is an alternative choice for the woman who does not wish to give birth in a hospital environment, yet is not comfortable giving birth at home. Birth centers do not provide any additional measure of safety than most planned home births with qualified midwives; they may provide the expectant couple with the physiological comfort necessary to enable the mother to relax.
Out-of-hospital birth centers are designed for women having low-risk pregnancies, who want drug-free birth with minimal intervention in a home-like environment. Family members may participate in the birth. C-sections rates are lower than most hospitals because the pregnancies are low risk. Freestanding Birth Centers are an alternative choice for a woman who has had a previous cesarean and wishes to maximize her chances of a vaginal delivery. However, vaginal birth attempts after a prior cesarean section have a 1-2% risk of uterine rupture. Health insurance may cover costs. Many birth centers offer birthing tubs where one can give birth in water.
Homebirth
Birth at home provides parents with intimacy, privacy, comfort and family-centered experience. Childbirth at home may be a safe option for healthy women having normal pregnancies. It is for those who have a very strong desire for natural childbirth, and who are willing to take a high degree of responsibility for their health care and baby’s birth. At home, the parents and midwife are in control of the birthing environment, and strict time perimeters for length of labor are not imposed, or routine medical interventions such as IVs done. In choosing the comfort of, home parents are also choosing to be further away from lifesaving measures, should complications arise.
Homebirth midwives provide complete prenatal care including monthly visits, laboratory tests, screening for infections. They provide nutritional counseling and support for psycho-social issues. There is a chance that a rare, but critical emergency might occur during the birth where hospital services may not be able to be obtained quick enough. Home birth midwives are trained to know when an emergency requires a medical interface, and can provide stabilizing measures until critical care can be obtained.

Complications during birth
Low birth weight
We have been discussing a number of teratogens associated with low birth weight such as cocaine, tobacco, etc. A child is considered low birth weight if he or she weighs less than 5.8 pounds (2500 grams). About 8.2 percent of babies born in the United States are of low birth weight (Center for Disease Control, 2010). A low birth weight baby has difficulty maintaining adequate body temperature because it lacks the fat that would otherwise provide insulation. Such a baby is also at more risk for infection. And 67 percent of these babies are also preterm which can make them more at risk for respiratory infection. Very low birth weight babies (2 pounds or less) have an increased risk of developing cerebral palsy. Many causes of low birth weight are preventable with proper prenatal care, however.
Premature birth
A child might also have a low birth weight if it is born at less than 37 weeks gestation (which qualifies it as a preterm baby). Early birth can be triggered by anything that disrupts the mother’s system. For instance, vaginal infections or gum disease can actually lead to premature birth because such infection causes the mother to release anti-inflammatory chemicals which, in turn, can trigger contractions. Smoking and the use of other teratogens can lead to preterm birth.
Anoxia
Anoxia is a temporary lack of oxygen to the brain. Difficulty during delivery may lead to anoxia which can result in brain damage or in severe cases, death. Babies who suffer both low birth weight and anoxia are more likely to suffer learning disabilities later in life as well.
Maternal and Infant Mortality
Approximately 1000 women die in childbirth around the world each day (World Health Organization, 2010). Rates are highest in Subsaharan Africa and South Asia although there has been a substantial decrease in these rates. The campaign in these regions to make childbirth safe has led to the development of clinics accessible to those living in more isolated areas and training more midwives to assist in childbirth.
LISTEN TO THIS NPR story, and/or read the transcript, about a midwife’s experience in a remote region of Afghanistan: In Afghanistan, Midwives ‘Are Like Guardian Angels For Infants And Mothers’
Infant mortality is the death of an infant before their first birthday. The infant mortality rate is the number of infant deaths for every 1,000 live births” (CDC N.d.). In 2020, Unicef ranked the United States 50th globally for infant mortality rate. (Unicef N.d.). Iceland has the lowest infant mortality rate at 1.54, while Sierra Leone has the highest at 80.10 deaths. (World Population Review N.d.b).
According to the CDC, the number of reported pregnancy-related deaths in the United States steadily increased from 7.2 deaths per 100,000 live births in 1987 to 32.9 deaths per 100,000 live births in 2021. Even in a highly industrialized nation with advanced technology, the United States faces a disparity issue in its infant mortality rates based on race.
WATCH THIS Historical and sociocultural explanations of infant and maternal mortality are discussed in the video clip below (or watch online):
READ THIS Read the linked article by Bani Saluga, MPH and Zenobia Bryant, Ph.D. (2021) published in the Journal of Women’s Health to learn more about how biases held by health care providers contribute to the United State’s poor maternal mortality rates. How Implicit Bias Contributes to Racial Disparities in Maternal Morbidity and Mortality in the United States.
Postpartum Care
For the pregnant person, if vaginal or perineum tearing occurs, or an episiotomy occurs the wound is closed with absorbable sutures. They should be closely watched for blood loss, infection, or any other possible complications. Breastfeeding should be initiated if possible soon after delivery, as the stimulation of oxytocin in the breastfeeding person aids in hemostasis.
After the baby is born, the umbilical cord is clamped and cut and the baby is assessed by a doctor, nurse practitioner, nurse midwife or nurse. There are several ways to assess the condition of the newborn. The most widely used tool is the Neonatal Behavioral Assessment Scale (NBAS) developed by T. Berry Brazelton. This tool has been used around the world to help parents get to know their infants and to make comparisons of infants in different cultures (Brazelton & Nugent, 1995). The baby’s motor development, muscle tone, and stress response are assessed. The APGAR developed by Dr. Virginia Apgar in 1952 is conducted one minute and five minutes after birth. Five things are assessed: the heart rate, respiration, muscle tone (quickly assessed by a skilled nurse when the baby is handed to them or by touching the baby’s palm), reflex response, and color. A score of 0 to 2 is given on each feature examined. A total APGAR of 5 or less is cause for concern. Scores of 8 or above are normal. The second APGAR should indicate improvement with a higher score.
WATCH THIS Watch an APGAR being done in the video clip below or online with captions:
|
Summary of the APGAR score chart. Adapted from: https://litfl.com/apg |
|||
|
Score |
0 Points |
1 Point |
2 Points |
|
Appearance – Skin Color |
Cyanotic/Pale all over (0 points) |
Peripheral cyanosis only (1 point) |
Pink (2 points) |
|
Pulse (Heart Rate) |
0 (0 points) |
<100 (1 point) |
100-140 (2 points) |
|
Grimace – Reflex irritability |
No response to stimulation (0 points) |
Grimace (facial movement)/weak cry when stimulated (1 point) |
Cry when stimulated (2 points) |
|
Activity – Tone |
Floppy (0 points) |
Some flexion (1 point) |
Well flexed and resisting extension (2 points) |
|
Respiration |
Apneic (0 points) |
Slow, irregular breathing (1 point) |
Strong cry (2 points) |
Skin to Skin Contact After Birth
Skin to skin contact is highly recommended for all infants especially within the first hour after birth (Feldman, Weller, Sirota, & Eidelman, 2002). Skin to skin refers to the parent, most typically the birthing person, having skin contact with the newborn. There are benefits of skin to skin contact between the birthing person and infant, psychosocially, physically, behaviorally, and neurobehavioral (Widström, Brimdyr, Svensson, Cadwell, & Nissen, 2019). The new parent can feel lower stress levels as does the baby. Through skin to skin contact the infant can self-regulate which is extremely helpful for those that were born premature or with a lower birth weight (Feldman et al.). Another term for skin to skin contact used by medical professionals is Kangaroo Care. Skin to skin or Kangaroo care is beneficial for premature babies as they have lost time to finish developing in the womb(Dabrowski, 2007). A review of previous research shows that Kangaroo Care has a positive effect on growth of the very low birth weight infants and also leads to increase in breast-feeding rates (Sharma, Farahbakhsh, Sharma, Sharma, & Sharma, 2019).
Birthing Practices Around the World
Birth is one thing that all human beings share in common, although birth experiences are all unique. Birth is a biosocial process influenced by the society and culture we live in. In addition to varied birth practices, there is wide cultural variation in beliefs about birth. For birth attendance, there is little variation in traditional cultures in who assists with the birth as it is rare for the male to be the primary support during birth. The father may help support the birth mother in various positions and other women in the room may be relatives. Here are a few other differences you might find in traditional cultures: Women from some cultures avoid moving too much during birth; some stay lying down, some prefer to sit or squat. After the birth, some women follow strict rules, such as staying in bed for several days.
SEE THIS Check out delivery trends across the world here (UNICEF data, July 2022).
Here are a few pregnancy practices across the world (Boules, 2020):
|
Region of the world |
Pregnancy |
During & after birth |
|
Afghanistan |
During the pregnancy the father did not play any role. |
The Placenta is buried in dark red ground. |
|
Cambodia |
During pregnancy, women avoid exposure to wind and wear warm clothes. |
The Cambodian Mothers prefer a female doctor for privacy with more body exposure. |
|
China |
A pregnant woman should not touch dirty things and not go to dirty places; they should be getting rest and having good food. |
Traditionally, husband will not be present during the birth Chinese mothers prefer to give birth in a sitting or squatting position. The new mother rests for one month cared for by the family who limit her dietary and behavior restrictions like limiting showers and eating only warm foods. |
READ THIS For more information check out this handout from Boules (2020).
The Postpartum Period
As the saying goes, it takes nine months for the baby to grow, so it is going to take time for a woman’s body to recover after birth. We live in a culture where movie and music stars give birth and show off their flat stomachs within days. This is so unfortunate as it places pressure on all American women to do the same. The information in this section provides realistic information regarding the postpartum period.
Getting Rest
The first few days at home after having a baby are a time for rest and recovery — physically and emotionally. A woman needs to focus her energy on herself and on getting to know her new baby. Even though she may be very excited and have requests for lots of visits from family and friends, she should try to limit visitors and get as much rest as possible. Women should not expect to keep their house perfect. New moms often find that all they can do is eat, sleep, and care for their baby. And that is perfectly okay. New moms should try to lie down or nap while the baby naps. They should allow others to help and not be afraid to ask for help with cleaning, laundry, meals, or with caring for the baby.
Physical Changes
Here is a list of common physical changes and experiences that occur after birth:
There is a vaginal discharge called lochia. It is the tissue and blood that lined the uterus during pregnancy.
It is heavy and bright red at first, becoming lighter in flow and color until it goes aware after a few weeks.
There may be swelling in the legs and feet.
Constipation may be experienced.
Menstrual-like cramping is common, especially if the woman is breastfeeding. The breast milk comes in within three to six days after delivery.
The woman’s doctor checks a woman’s recovery at a postpartum visit, about six weeks after birth. Some women develop thyroid problems in the first year after giving birth. This is called postpartum thyroiditis. It often begins with overactive thyroid, which lasts two to four months. Most women then develop symptoms of an underactive thyroid, which can last up to a year. Thyroid problems are easy to overlook, as many symptoms, such as fatigue, sleep problems, low energy, and changes in weight, are common after having a baby. In most cases, thyroid function returns to normal as the thyroid heals. But some women develop permanent underactive thyroid disease, called Hashimoto’s disease, and need lifelong treatment.
Regaining a Healthy Weight
Both pregnancy and labor can affect a woman’s body. After giving birth, women lose about 10 pounds right away and a little more as body fluid levels decrease. Women should not expect or try to lose additional pregnancy weight right away. Gradual weight loss over several months is the safest way, especially if breastfeeding. Nursing mothers can safely lose a moderate amount of weight without affecting their milk supply or their babies’ growth.
Baby Blues and Postpartum Depression
After childbirth, women may feel sad, weepy, and overwhelmed for a few days. Many new mothers have the “baby blues” after giving birth. Changing hormones, anxiety about caring for the baby, and lack of sleep, all affect emotions.
Baby blues are common due to rapid hormonal changes but resolve after 1-2 weeks. These feelings are normal and usually go away quickly. But if sadness lasts more than two weeks, the new mother may have a serious but treatable condition called postpartum depression. Postpartum depression can happen any time within the first year after birth.
Postpartum depression affects approximately 10 to 15 percent of new mothers. It often causes anxiety and obsession about caring for the baby or the cleanliness of the home. It may cause changes in sleep patterns and affect relationships, including the ability to form a bond with the baby and other family members. Some mothers with postpartum depression have thoughts of wanting to die or of hurting the baby. Postpartum depression is characterized by persisting symptoms, and the mother should notify her provider immediately.
Signs of postpartum depression include:
- Feeling restless or irritable
- Feeling sad, depressed, or crying a lot
- Having no energy
- Having headaches, chest pains, heart palpitations (the heart being fast and feeling like it is skipping beats) numbness, or hyperventilation (fast and shallow breathing)
- Not being able to sleep, being very tired, or both
- Not being able to eat and weight loss
- Overeating and weight gain
- Trouble focusing, remembering, or making decisions
- Being overly worried about the baby
- Not having any interest in the baby
- Feeling worthless and guilty
- Having no interest or getting no pleasure from activities like sex and socializing
- Thoughts of harming your baby or yourself
Some women don’t tell anyone about their symptoms because they feel embarrassed or guilty about having these feelings at a time when they think they should be happy. Postpartum depression can make it hard to take care of the baby. Infants with mothers with postpartum depression can have delays in learning how to talk. They can have problems with emotional bonding. Therapy and/or medicine can treat postpartum depression.
Emerging research suggests that 1 in 10 new fathers may experience depression during or after pregnancy. Although more research is needed, having depression may make it harder to be a good father and perhaps affect the baby’s development. Having depression may also be related to a mother’s depression. New fathers with emotional problems or symptoms of depression should talk to their doctors. Depression is a treatable illness.
CLICK OR CALL THIS: If you or someone you know is experiencing symptoms of depression or just needs someone to talk to about a new pregnancy or birth, The National Maternal Mental Health Hotline through the US government’s Health Resources and Services Administration is free, confidential, and here to help 24/7. You can call (1-833-TLC-MAMA), text or contact them through their website and speak with a trained counselor in English or Spanish.
Making a Family
It’s important to recognize there are numerous pathways to parenthood. For many, methods such as in vitro fertilization (IVF) and adoption provide solutions for those facing reproductive challenges. They also create opportunities for diverse family structures and experiences, enriching the narrative of what it means to become a parent. Below are some, though not all, ways people welcome children into their families.
Foster Care, Guardianships, and Adoption
Foster Care
The foster care system has been around for years. According to The National Foster Parent Association, the United States foster care system developed from the English Poor Law of 1562. This law stated that children from poor homes would enter into indentured services until they were at an age in which they could care for themselves. The first child in the US to enter into the foster care system was in 1636, and he went by the name Benjamin Eaton. Charles Loring Brace was the first to initiate a free foster home movement in 1853.
READ THIS for more information about the history of foster care and much more, visit the University of Oregon’s The Adoption History Project.
Today foster care is known as a temporary placement in which children who have been removed from their families take up residence either with other family members (first choice, or non-relatives (alternative if no family is able or available to step in). Foster care can be done through government agencies or non-governmental organizations.
Steps to Become a Foster Parents
There are many steps to take to become a foster parent. The Michigan DHHS website lists five steps that have to be completed in order for anyone to become official foster parents. These steps are listed below:
Call a Navigator: Foster Care Navigators are experienced foster parents who can answer questions and find an agency.
Attend an Orientation: Review guidelines, illustrate what to expect, and has representatives to help answer questions.
Complete Application: agency chosen provides a licensing application packet (one must be licensed in order to officially become a foster parent). Refer to link to learn more about the application process.
Participate in a Home Evaluation: Have to pass an on-site home evaluation performed by licensing agent. Interviews and home visits will be done multiple times.
Attend Free Training: Agency will schedule a PRIDE (Parent Resources for Information Development and Education) training with the prospective foster parent. Must complete 12 hours and once they are licensed they have 18 months to go through it again.
Guardianships
With permanency being the goal, guardianship is one way to help provide permanency to children who may or may not be able to return home. This option provides permanency yet allows the parents to still have access to the child through visitation. For this process, there is a court hearing and the court decides if the potential guardians are deemed appropriate. They have to pass home visits and more, just like a foster parent. Anyone can be a guardian, but it is common for other family members to apply for guardianships to help avoid the child having to go to people who are not within the family system.
Adoption
Adopting a child can take various forms, each with its own processes and considerations. The main types of adoption include:
Domestic Adoption: Adoption within the adoptive and birth parents’ home country.
Private Adoption: Arranged through an adoption agency or directly between adoptive and birth parents.
Public Adoption: Involves children in the foster care system and is typically managed by state or local child welfare agencies.
International Adoption: Involves adopting a child from a different country, governed by international laws and the regulations of both the child’s home country and the adoptive parents’ country.
Relative Adoption (Kinship Adoption): Adopting a child who is a relative, such as a grandchild, niece, or nephew. This can provide continuity and stability for the child.
Stepparent Adoption: A stepparent adopts their spouse’s biological child, legally solidifying the parent-child relationship.
Open Adoption: Allows for some form of communication or contact between the birth parents, adoptive parents, and the child, ranging from letters and photos to regular visits.
Closed Adoption: No contact or identifying information is shared between birth parents and adoptive parents. The child’s adoption records are typically sealed.
Foster-to-Adopt: Children are initially placed in foster care with the intention of adoption. This can provide a path to permanency for children in the foster care system.
Each type of adoption has its unique legal requirements, emotional considerations, and procedural steps, making it essential for prospective adoptive parents to thoroughly research and understand the process that best fits their situation and needs.
READ THIS For more information on how adoption affects the adoptive parent(s), birth parents, and adoptees, see the article “What does adoption mean?” by the company American Adoptions.
In vitro fertilization
In vitro fertilization (IVF) is a technique in which egg cells are fertilized by sperm outside the woman’s womb. IVF is a major treatment in infertility when other methods of achieving conception have failed. The process involves hormonally controlling the ovulatory process, removing ova (eggs) from the woman’s ovaries and letting sperm fertilize them in a fluid medium. The fertilized egg (zygote) is then transferred to the patient’s uterus with the intent to establish a successful pregnancy.
The term in vitro, is used, because early biological experiments involving cultivation of tissues outside the living organism from which they came, were carried out in glass containers such as beakers, test tubes, or petri dishes.
While the overall live birth rate via IVF in the U.S. is about 27% per cycle (33% pregnancy rate), the chances of a successful pregnancy via IVF vary widely based on the age of the woman (or, more precisely, on the age of the eggs involved). Where the woman’s own eggs are used as opposed to those of a donor, for women under 35, the pregnancy rate is commonly approximately 43% per cycle (37% live birth), while for women over 40, the rate falls drastically – to only 4% for women over 42. Other factors that determine success rates include the quality of the eggs and sperm, the duration of the infertility, the health of the uterus, and the medical expertise. It is a common practice for IVF programs to boost the pregnancy rate by placing multiple embryos during embryo transfer. A flip side of this practice is a higher risk of multiple pregnancy, which is associated with obstetric complications.
Embryo cryopreservation If multiple embryos are generated, patients may choose to freeze embryos that are not transferred. Those embryos are placed in liquid nitrogen and can be preserved for a long time. There are currently 500,000 frozen embryos in the United States. The advantage is that patients who fail to conceive may become pregnant using such embryos without having to go through a full IVF cycle. Or, if pregnancy occurred, they could return later for another pregnancy.
Surrogacy
Surrogacy, the situation where a person intentionally gets pregnant and carries a child for someone else, began flourishing in the USA in the 1980s, and today it has grown into a global trend. Sometimes arrangements are non-paid, but often they are contracted and paid. In traditional or partial surrogacy, the surrogate’s own eggs are used, making the surrogate and the surrogacy-conceived child genetically related. In gestational or full surrogacy, the egg of either the intended parent or an egg-donor is used.
READ THIS For more information on the steps to surrogacy, read the article “The Six Steps of the Surrogacy Process” from Surrogate.com.
References and Resources
Listed below are the references and resources used to curate this module.
Gunnarsson Payne, J., Korolczuk, E., & Mezinska, S. (2020). Surrogacy relationships: a critical interpretative review. Upsala journal of medical sciences, 125(2), 183–191. https://doi.org/10.1080/03009734.2020.1725935 (“Surrogacy”)
Iowa State University. (n.d.). Hereditary. In Individual and family development. Retrieved from https://iastate.pressbooks.pub/individualfamilydevelopment/chapter/hereditary/
LibreTexts. (n.d.). Labor and birth. In Sexuality, the self, and society. Retrieved from https://socialsci.libretexts.org/Bookshelves/Gender_Studies/Sexuality_the_Self_and_Society_(Ruhman_Bowman_Jackson_Lushtak_Newman_and_Sunder)/10%3A_Conception_Pregnancy_and_Childbirth/10.08%3A_Labor_and_Birth
LibreTexts. (n.d.). The newborn, APGAR score, and postpartum period. In Child and adolescent psychology. Retrieved from https://socialsci.libretexts.org/Courses/Lumen_Learning/Book%3A_Child_and_Adolescent_Psychology_(Lumen)/4%3A_Module_2%3A_The_Dawn_of_a_Person/4.6%3A_The_Newborn_APGAR_Score_and_Postpartum_Period
Lumen Learning. (n.d.). Behavioral genetics. In Lifespan development. Retrieved from https://courses.lumenlearning.com/suny-lifespandevelopment/chapter/behavioral-genetics/
Lumen Learning. (n.d.). Chromosomal abnormalities and genetic testing. In Lifespan development. Retrieved from https://courses.lumenlearning.com/wm-lifespandevelopment/chapter/chromosomal-abnormalities-and-genetic-testing/
Lumen Learning. (n.d.). Environmental risks during prenatal development. In Lifespan development. Retrieved from https://courses.lumenlearning.com/wm-lifespandevelopment/chapter/environmental-risks-during-prenatal-development/
Lumen Learning. (n.d.). Genetic disorders. In Lifespan development. Retrieved from https://courses.lumenlearning.com/suny-lifespandevelopment/chapter/genetic-disorders/
Lumen Learning. (n.d.). Heredity. In Lifespan development. Retrieved from https://courses.lumenlearning.com/suny-lifespandevelopment/chapter/heredity/
Lumen Learning. (n.d.). Introduction. In Lifespan development. Retrieved from https://courses.lumenlearning.com/suny-lifespandevelopment/chapter/introduction-2/
Lumen Learning. (n.d.). Prenatal development. In Lifespan development. Retrieved from https://courses.lumenlearning.com/wm-lifespandevelopment/chapter/prenatal-development/
Maricopa Community Colleges. (n.d.). Heredity, prenatal development, and birth. In PSY 240: Developmental psychology. Retrieved from https://open.maricopa.edu/psy240mm/chapter/chapter-3-heredity-prenatal-development-and-birth-2/
Noba Project. (n.d.). The nature-nurture question. Retrieved from https://nobaproject.com/modules/the-nature-nurture-question
Nova Scotia Community College. (n.d.). Pregnancy and childbirth. In Developmental psychology: An introduction. Retrieved from https://pressbooks.nscc.ca/devpsychology/chapter/pregnancy-and-childbirth/
Open Washington. (n.d.). Health and illness in the United States. In Introduction to sociology. Retrieved from https://openwa.pressbooks.pub/sccsoci101/chapter/18-3-health-and-illness-in-the-united-states/
Reigstad, B and OpenAI. (2024). “Types of adoption” written and edited by first author using GPT-4o (May 24 version) [Large language model]. https://chat.openai.com
