
10 Module 10: Middle Adulthood Development
Module 10 Learning Objectives
Upon completion of this module, the learner will be able to:
- Describe Physical Changes
Explain the key physiological changes that occur during middle adulthood, including vision, hearing, and metabolism. - Understand Chronic Health Concerns
Discuss the impact of conditions such as osteoporosis, sarcopenia, and chronic inflammation on quality of life in adulthood. - Examine Hormonal Changes
Summarize the effects of menopause and andropause on physical and emotional health in middle adulthood. - Discuss Cognitive Development
Differentiate between fluid and crystallized intelligence and describe how they change during adulthood. - Explore Erikson’s Psychosocial Theory
Explain the crisis of generativity vs. stagnation and its role in middle adulthood development. - Analyze Work Satisfaction
Discuss factors influencing job satisfaction and productivity, including personality traits and workplace relationships. - Understand Relationships in Adulthood
Describe changes in intimate, familial, and workplace relationships during middle adulthood. - Evaluate the Sandwich Generation
Explain the challenges faced by middle-aged adults caring for both children and aging parents. - Examine Socioemotional Selectivity Theory
Understand how shifting time perspectives influence emotional and social priorities in middle adulthood. - Recognize Cultural Variations
Discuss how cultural expectations and norms affect the experience of middle adulthood, including health and family roles. - Identify Strategies for Successful Aging
Explain the selection, optimization, and compensation model and its application to maintaining quality of life. - Discuss Midlife Transitions
Evaluate the concept of the midlife crisis and its relevance to personal growth and life satisfaction.
Physical Development
Physical Mobility in Middle Adulthood
The importance of not succumbing to the temptations of a sedentary lifestyle was as obvious to Hippocrates in 400 BCE as it is now. Piasecki et al (2018) are of the opinion that sarcopenia (loss of muscle tissue and function as we age) in legs might be the result of leg muscles becoming detached from the nervous system. Further, Piasescki et al (2018) believe that exercise encourages new nerve growth slowing the progression of sarcopenia. Persons aged 75 may have up to 30-60% fewer nerve endings in their leg muscles than they did in their early 20s.

Sarcopenia has only recently been recognized as an independent disease entity since 2016 (ICD-10). In 2018 the U.S. Center for Disease Control and prevention assigned sarcopenia its own discrete medical code. Disease entities that affect mobility will become an increasingly costly phenomenon, and will affect the quality of life of millions of people as the population ages. In many ways it is a natural phenomenon, and many doctors and researchers have been reticent to overly pathologize natural changes associated with age. However, mobility is now becoming a central concern, and some researchers are now identifying some conditions like osteosarcopenia, which describes the decline of both muscle tissue (sarcopenia) and bone tissue (osteoporosis). Diagnoses and pharmaceuticals which deal with the central question of mobility will become ever more important, even more so as the burgeoning costs associated with caring for those with mobility issues becomes apparent.
The years between 30 and 60 can see the onset of rheumatoid arthritis (RA). This is the third most common form of arthritis and its specific etiology is unknown at this time. RA occurs when antibodies attack normal synovial fluid in the joints mistaking them for an alien threat. It affects women more than men by a factor of around 3 to 1. Peak onset for women is reckoned to be sometime in the early 40s. This has led to the conclusion, albeit a preliminary one, that RA is caused by hormonal changes. Women who are pregnant, and have RA, often experience a temporary remission, again leading to the identification of hormonal changes in the body as the most likely culprit. Women also experience symptoms at an earlier age. This condition is often associated with people in their 60s, but only about a third first experience symptoms at this age, though they become more acute with the passage of time.
Human beings reach peak bone mass around 35-40. Osteoporosis is a “silent disease” which progresses until a fracture occurs. The sheer scale and cost of this illness is radically underestimated. It is often associated with women due to the fact that bone mass can deteriorate in women much more quickly in middle age due to menopause. After menopause women can lose 5-10% bone mass per year, rendering it advisable to monitor intakes of calcium and Vitamin D, and evaluate individual risk factors. Beginning in their 60s, though, men and women lose bone mass at roughly the same rate. The number of American men diagnosed with osteoporosis is currently around the 2 million mark, with a further 12 million reckoned to be at risk. The National Osteoporosis Foundation (NOF) estimates that 50% of women and 25% of men over the age of 50 will suffer a bone fracture due to osteoporosis. Attention at this stage of the life may bring pronounced health benefits now and later for both women and men. Fixing the damage takes a considerable amount of the Medicare budget.
The health benefits that walking and other physical activity have on the nervous system are becoming increasingly obvious to those who study aging. Adami et al (2018) found pronounced links between weight bearing exercise and neuron production. We tend to think of the brain as a central processing unit giving instructions to the body via the conduit of the central nervous system, but contemporary science is now coalescing around the idea that muscles and nerves also communicate with the brain—it is a two-way informational and sustaining process. Many studies suggest that voluntary physical activity (VPA) extends and improves quality of life. Such studies show that even moderate physical activity can bring large gains.
In addition, there is often an increase in chronic inflammation at this time of life with no discernible discrete cause (as opposed to acute inflammation associated with something like an infection). Inflammation is the body’s natural way of responding to injury or harmful pathogens in the body. The function of inflammation is to eliminate the initial cause of injury and initiate tissue repair, but when this happens consistently and for longer periods of time, the body’s stress response systems become overworked. This can have serious effects on health, such as fatigue, fever, chest or abdominal pain, rashes, or greater susceptibility to diseases such as cancer, rheumatoid arthritis, and heart disease. Untreated acute inflammation, autoimmune disorders, or long-term exposure to irritants are some contributing factors, as is social isolation (Nersessian et al, 2018).
Chronic inflammation has been implicated as part of the cause of the muscle loss that occurs with aging. Chronic inflammatory disorder is now implicated in a whole series of chronic diseases such as dementia, and the biomedical evidence for its centrality is now emerging in the medical research literature.
Because of the aging population, health issues associated with autoimmune disease, chronic inflammation, and bone mass density will become central concerns in health and social policy in the coming decades.
Normal Physiological Changes in Middle Adulthood
There are a few primary biological physical changes in midlife. There are changes in vision, hearing, more joint pain, and weight gain (Lachman, 2004). Vision is affected by age. As we age, the lens of the eye gets larger but the eye loses some of the flexibility required to adjust to visual stimuli. This is known as presbyopia. Middle aged adults often have trouble seeing up close as a result. Night vision is also affected as the pupil loses some of its ability to open and close to accommodate drastic changes in light.
Presbycusis is the most common cause of hearing loss, afflicting one out of four persons between ages 65 and 74, and one out of two by age 75. This loss accumulates after years of being exposed to intense noise levels, and is generally due to the loss or damage of nerve hair cells inside the cochlea. It is more common in men, but men are also more likely to work in noisy occupations, which may explain their nearly doubled rates of hearing loss levels. Hearing loss is also exacerbated by cigarette smoking, high blood pressure, and stroke. High frequency sounds are the first affected by such hearing loss. Hearing loss could be prevented by guarding against being exposed to extremely noisy environments.
There is new concern over hearing loss as early as childhood with the widespread use of headphones, as loud and/or prolonged listening can cause damage to the cilia, or the tiny sensory hairs, within the cochlea. Another cause of hearing loss in middle age is otosclerosis, a physiological condition affecting the middle ear and its bone structure. This occurs when one of the bones in the middle ear, the stapes, acquires a rigidity via abnormal bone growth which it should not have. Unable to vibrate, it induces hearing impairment. Otosclerosis is often described as a rare condition, but it afflicts a good number of Americans, with white women being more prone, though there has been some speculation that this was the origin of deafness in the composer Beethoven. Its cause is unknown, but chronic inflammation may be a risk factor. We tend to associate hearing loss with older adults, but peak onset is in the middle adulthood age bracket.
Weight gain, sometimes referred to as the middle-aged spread, or the accumulation of fat in the abdomen is one of the common complaints of midlife adults. Men tend to gain fat on their upper abdomen and back while women tend to gain more fat on their waist and upper arms. Many adults are surprised at this weight gain because their diets have not changed. However, the metabolism slows by about one-third during midlife (Berger, 2005). Consequently, midlife adults have to increase their level of exercise, eat less, and watch their nutrition to maintain their earlier physique.
Many of the changes that occur in midlife can be easily compensated for (by buying glasses, exercising, and watching what one eats, for example.) Most midlife adults experience generally good health. However, the percentage of adults who have a disability increases through midlife; while 7 percent of people in their early 40s have a disability, the rate jumps to 30 percent by the early 60s. This increase is highest among those of lower socioeconomic status (Bumpass and Aquilino, 1995).
What can we conclude from this information? Again, lifestyle has a strong impact on the health status of midlife adults. Smoking tobacco, drinking alcohol, poor diet, stress, physical inactivity, and chronic disease such as diabetes or arthritis reduce overall health. It becomes important for midlife adults to take preventative measures to enhance physical well-being. Those midlife adults who have a strong sense of mastery and control over their lives, who engage in challenging physical and mental activity, who engage in weight bearing exercise, monitor their nutrition, and make use of social resources are most likely to enjoy a plateau of good health through these years. Not only that, but those who begin an exercise regimen in their 40s may enjoy comparable benefits to those who began in their 20s according to Saint-Maurice et al (2019), who also found that while it is never too late to begin, continuing to do as much as possible, is just as important.
The Climacteric
One biologically based change that occurs during midlife is the climacteric. During midlife, men may experience a reduction in their ability to reproduce. Women, however, lose their ability to reproduce once they reach menopause.
Menopause
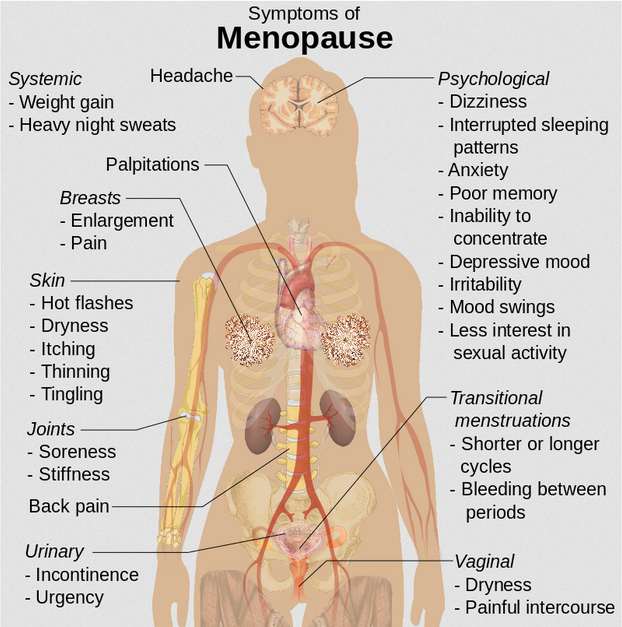
Menopause refers to a period of transition in which a woman’s ovaries stop releasing eggs and the level of estrogen and progesterone production decreases. After menopause, a woman’s menstruation ceases.
Changes typically occur between the mid 40s and mid 50s. The median age range for a woman to have her last menstrual period is 50-52, but ages vary. A woman may first begin to notice that her periods are more or less frequent than before. These changes in menstruation may last from 1 to 3 years. After a year without menstruation, a woman is considered menopausal and no longer capable of reproduction. (Keep in mind that some women, however, may experience another period even after going for a year without one.) The loss of estrogen also affects vaginal lubrication which diminishes and becomes more watery. The vaginal wall also becomes thinner, and less elastic.
Menopause is not seen as universally distressing (Lachman, 2004). Changes in hormone levels are associated with hot flashes and sweats in some women, but women vary in the extent to which these are experienced. Depression, irritability, and weight gain are not necessarily due to menopause (Avis, 1999; Rossi, 2004). Depression and mood swings are more common during menopause in women who have prior histories of these conditions rather than those who have not. The incidence of depression and mood swings is not greater among menopausal women than non-menopausal women.
Cultural influences seem to also play a role in the way menopause is experienced. For example, once after listing the symptoms of menopause in a psychology course, a woman from Kenya responded, “We do not have this in my country or if we do, it is not a big deal,” to which some U.S. students replied, “I want to go there!” Indeed, there are cultural variations in the experience of menopausal symptoms. Hot flashes are experienced by 75 percent of women in Western cultures, but by less than 20 percent of women in Japan (Obermeyer in Berk, 2007).
Women in the United States respond differently to menopause depending upon the expectations they have for themselves and their lives. White, African-American, Mexican-American, and career-oriented women overall tend to think of menopause as a liberating experience. Nevertheless, there has been a popular tendency to erroneously attribute frustrations and irritations expressed by women of menopausal age to menopause and thereby not take her concerns seriously. Fortunately, many practitioners in the United States today are normalizing rather than pathologizing menopause.
Concerns about the effects of hormone replacement have changed the frequency with which estrogen replacement and hormone replacement therapies have been prescribed for menopausal women. Estrogen replacement therapy was once commonly used to treat menopausal symptoms. But more recently, hormone replacement therapy has been associated with breast cancer, stroke, and the development of blood clots (NLM/NIH, 2007). Most women do not have symptoms severe enough to warrant estrogen or hormone replacement therapy (HRT). Women who do require HRT can be treated with lower doses of estrogen and monitored with more frequent breast and pelvic exams. There are also some other ways to reduce symptoms. These include avoiding caffeine and alcohol, eating soy, remaining sexually active, practicing relaxation techniques, and using water-based lubricants during intercourse.
Fifty million women in the USA aged 50-55 are post-menopausal. During and after menopause a majority of women will experience weight gain. Changes in estrogen levels lead to a redistribution of body fat from hips and back to stomachs. This is more dangerous to general health and wellbeing because abdominal fat is largely visceral, meaning it is contained within the abdominal cavity and may not look like typical weight gain. That is, it accumulates in the space between the liver, intestines and other vital organs. This is far more harmful to health than subcutaneous fat which is the kind of fat located under the skin. It is possible to be relatively thin and retain a high level of visceral fat, yet this type of fat is deemed especially harmful by medical research.
Andropause
Do males experience a climacteric? Yes. While they do not lose their ability to reproduce as they age, they do tend to produce lower levels of testosterone and fewer sperm. However, men are capable of reproduction throughout life after puberty. It is natural for sex drive to diminish slightly as men age, but a lack of sex drive may be a result of extremely low levels of testosterone. About 5 million men experience low levels of testosterone that results in symptoms such as a loss of interest in sex, loss of body hair, difficulty achieving or maintaining erection, loss of muscle mass, and breast enlargement. This decrease in libido and lower testosterone (androgen) levels is known as andropause, although this term is somewhat controversial as this experience is not clearly delineated, as menopause is for women. Low testosterone levels may be due to glandular disease such as testicular cancer. Testosterone levels can be tested and if they are low, men can be treated with testosterone replacement therapy. This can increase sex drive, muscle mass, and beard growth. However, long term HRT for men can increase the risk of prostate cancer (The Patient Education Institute, 2005).
The debate around declining testosterone levels in men may hide a fundamental fact. The issue is not about individual males experiencing individual hormonal change at all. We have all seen the adverts on the media promoting substances to boost testosterone: “Is it low-T?” The answer is probably in the affirmative, if somewhat relative. That is, in all likelihood they will have lower testosterone levels than their fathers. However, it is equally likely that the issue does not lie solely in their individual physiological make up, but is rather a generational transformation (Travison et al, 2007).
Why this has occurred in such a dramatic fashion is still unknown. There is evidence that low testosterone may have negative health effects on men. In addition, there are studies which show evidence of rapidly decreasing sperm count and grip strength. Exactly why these changes are happening is unknown and will likely involve more than one cause.
The Climacteric and Sexuality
Sexuality is an important part of people’s lives at any age. Midlife adults tend to have sex lives that are very similar to that of younger adulthood. And many women feel freer and less inhibited sexually as they age. However, a woman may notice less vaginal lubrication during arousal and men may experience changes in their erections from time to time. This is particularly true for men after age 65. Men who experience consistent problems are likely to have other medical conditions (such as diabetes or heart disease) that impact sexual functioning (National Institute on Aging, 2005).
Couples continue to enjoy physical intimacy and may engage in more foreplay, oral sex, and other forms of sexual expression rather than focusing as much on sexual intercourse. Risk of pregnancy continues until a woman has been without menstruation for at least 12 months, however, and couples should continue to use contraception. People continue to be at risk of contracting sexually transmitted infections such as genital herpes, chlamydia, and genital warts. About ten percent of new HIV diagnoses in the United States are in people 55 and older. Of all people living with HIV, almost 50% are aged 50 or over. Getting tested is important- even people who are not high-risk can be impacted. Also, practicing safe sex is important at any age- safe sex is not just about avoiding an unwanted pregnancy… it is about protecting yourself from STDs as well. Hopefully, when partners understand how aging affects sexual expression, they will be less likely to misinterpret these changes as a lack of sexual interest or displeasure in the partner and be more able to continue to have satisfying and safe sexual relationships.
Exercise, Nutrition, and Health
The impact of exercise
Exercise is a powerful way to combat the changes we associate with aging. Exercise builds muscle, increases metabolism, helps control blood sugar, increases bone density, and relieves stress. Unfortunately, fewer than half of midlife adults exercise and only about 20 percent exercise frequently and strenuously enough to achieve health benefits. Many stop exercising soon after they begin an exercise program-particularly those who are very overweight. The best exercise programs are those that are engaged in regularly—regardless of the activity, but a well-rounded program that is easy to follow includes walking and weight training. Having a safe, enjoyable place to walk can make the difference in whether or not someone walks regularly. Weight lifting and stretching exercises at home can also be part of an effective program. Exercise is particularly helpful in reducing stress in midlife. Walking, jogging, cycling, or swimming can release the tension caused by stressors, and learning relaxation techniques can have healthful benefits. Exercise can be thought of as preventative health care; promoting exercise for the 78 million “baby boomers” may be one of the best ways to reduce health care costs and improve quality of life.


Nutrition
Aging brings about a reduction in the number of calories a person requires. Many Americans respond to weight gain by dieting. However, eating less does not necessarily mean eating right and people often suffer vitamin and mineral deficiencies as a result. Very often, physicians will recommend vitamin supplements to their middle aged patients. As stated above, chronic inflammation is now identified as one of the so called “pillars of aging”. The link between diet and inflammation is somewhat still unclear, but research supports a diet rich in plant-based foods, healthy fats, nuts, fish in moderation, and sparing use of red meat— often referred to as “the Mediterranean Diet.”
The ideal diet is one low in fat, low in sugar, high in fiber, low in sodium, and low in cholesterol. In 2005, the Food Pyramid, a set of nutritional guidelines established by the U. S. Government was updated to accommodate new information on nutrition and to provide people with guidelines based on age, sex, and activity levels. The ideal diet is low in sodium (less than 2300 mg per day). Sodium causes fluid retention which may in turn exacerbate high blood pressure. The ideal diet is also low in cholesterol (less than 300 mg per day) and high in fiber. Fiber is thought to reduce the risk of certain cancers and heart disease. Finally, an ideal diet is low in sugar. Sugar is not only a problem for diabetics; it is also a problem for most people. Sugar satisfies the appetite but provides no protein, vitamins or minerals. It provides empty calories. High starch diets are also a problem because starch is converted to sugar in the body. A 1-2 ounce serving of red wine (or grape juice) may have beneficial effects on health, as red wine can increase “good cholesterol” or HDLs (high density lipoproteins) in the blood and provide antioxidants important for combating aging.
Cognitive Development in Middle Adulthood
One of the most influential perspectives on cognition during middle adulthood has been that of the Seattle Longitudinal Study (SLS) of adult cognition, which began in 1956. Schaie & Willis (2010) summarized the general findings from this series of studies as follows: “We have generally shown that reliably replicable average age decrements in psychometric abilities do not occur prior to age 60, but that such reliable decrement can be found for all abilities by 74 years of age.” In short, decreases in cognitive abilities begin in the sixth decade and gain increasing significance from that point on. However, Singh-Maoux et al (2012) argue for small but significant cognitive declines beginning as early as age 45. There is some evidence that adults should be as aggressive in maintaining their cognitive health as they are their physical health during this time as the two are intimately related.

CLICK THIS: The Seattle Longitudinal Study (SLS) is still running! Learn more about the study and read it’s most recent findings at it’s official website.
A second source of longitudinal research data on this part of the lifespan has been The Midlife in the United States Studies (MIDUS), which began in 1994. The MIDUS data supports the view that this period of life is something of a trade-off, with some cognitive and physical decreases of varying degrees. The cognitive mechanics of processing speed, often referred to as fluid intelligence, physiological lung capacity, and muscle mass, are in relative decline. However, knowledge, experience and the increased ability to regulate our emotions can compensate for these losses. Continuing cognitive focus and exercise can also reduce the extent and effects of cognitive decline.
CLICK THIS: The Midlife in the United States Studies (MIDUS) is still running! Learn more about the study, read it’s most recent findings, and even link to its dataset at the official website.
Control Beliefs
Central to all of this are personal control beliefs, which have a long history in psychology. Beginning with the work of Julian Rotter (1954), a fundamental distinction is drawn between those who believe that they are the fundamental agent of what happens in their life, and those who believe that they are largely at the mercy of external circumstances. Those who believe that life outcomes are dependent on what they say and do are said to have a strong internal locus of control. Those who believe that they have little control over their life outcomes are said to have an external locus of control.
Empirical research has shown that those with an internal locus of control enjoy better results in psychological tests across the board; behavioral, motivational, and cognitive. It is reported that this belief in control declines with age, but again, there is a great deal of individual variation. This raises another issue: directional causality. Does my belief in my ability to retain my intellectual skills and abilities at this time of life ensure better performance on a cognitive test compared to those who believe in their inexorable decline? Or, does the fact that I enjoy that intellectual competence or facility instill or reinforce that belief in control and controllable outcomes? It is not clear which factor is influencing the other. The exact nature of the connection between control beliefs and cognitive performance remains unclear.
Brain science is developing exponentially and will unquestionably deliver new insights on a whole range of issues related to cognition in midlife. One of them will surely be on the brain’s capacity to renew, or at least replenish itself, at this time of life. The capacity to renew is called neurogenesis; the capacity to replenish what is there is called neuroplasticity. At this stage, it is impossible to ascertain exactly what effect future pharmacological interventions may have on possible cognitive decline at this, and later, stages of life.
Cognitive Aging
Researchers have identified areas of loss and gain in cognition in older age. Cognitive ability and intelligence are often measured using standardized tests and validated measures. The psychometric approach has identified two categories of intelligence that show different rates of change across the life span (Schaie & Willis, 1996). Fluid and crystallized intelligence were first identified by Cattell in 1971. Fluid intelligence refers to information processing abilities, such as logical reasoning, remembering lists, spatial ability, and reaction time.

Crystallized intelligence encompasses abilities that draw upon experience and knowledge. Measures of crystallized intelligence include vocabulary tests, solving number problems, and understanding texts. There is a general acceptance that fluid intelligence decreases continually from the 20s, but that crystallized intelligence continues to accumulate. One might expect to complete the NY Times crossword more quickly at 48 than 22, but the capacity to deal with novel information declines.
WATCH THIS video below or online on Fluid and Crystallized Intelligence:
With age, systematic declines are observed on cognitive tasks requiring self-initiated, effortful processing, without the aid of supportive memory cues. Older adults tend to perform poorer than young adults on memory tasks that involve recall of information, where individuals must retrieve information they learned previously without the help of a list of possible choices. For example, older adults may have more difficulty recalling facts such as names or contextual details about where or when something happened. What might explain these deficits as we age?


As we age, working memory, or our ability to simultaneously store and use information, becomes less efficient (Craik & Bialystok, 2006). The ability to process information quickly also decreases with age. This slowing of processing speed may explain age differences on many different cognitive tasks (Salthouse, 2004). Some researchers have argued that inhibitory functioning, or the ability to focus on certain information while suppressing attention to less pertinent information, declines with age and may explain age differences in performance on cognitive tasks (Hasher & Zacks, 1988).
Fewer age differences are observed when memory cues are available, such as for recognition memory tasks, or when individuals can draw upon acquired knowledge or experience. For example, older adults often perform as well if not better than young adults on tests of word knowledge or vocabulary. With age often comes expertise, and research has pointed to areas where aging experts perform as well or better than younger individuals. For example, older typists were found to compensate for age-related declines in speed by looking farther ahead at printed text (Salthouse, 1984). Compared to younger players, older chess experts are able to focus on a smaller set of possible moves, leading to greater cognitive efficiency (Charness, 1981). Accrued knowledge of everyday tasks, such as grocery prices, can help older adults to make better decisions than young adults (Tentori, Osheron, Hasher, & May, 2001).
We began with Schaie and Willis (2010) observing that no discernible general cognitive decline could be observed before 60, but other studies contradict this notion. How do we explain this contradiction? In a thought-provoking article, Ramscar et al (2014) argued that an emphasis on information processing speed ignored the effect of the process of learning/experience itself; that is, that such tests ignore the fact that more information to process leads to slower processing in both computers and humans. We are more complex cognitive systems at 55 than 25.
WATCH THIS video below or online that highlights some of the cognitive changes during adulthood as well as the characteristics that either decline, improve, or remain stable:
Cognitive Performance in Middle Adulthood
Research on interpersonal problem solving suggests that older adults use more effective strategies than younger adults to navigate through social and emotional problems (Blanchard-Fields, 2007). In the context of work, researchers rarely find that older individuals perform less well on the job (Park & Gutchess, 2000). Similar to everyday problem solving, older workers may develop more efficient strategies and rely on expertise to compensate for cognitive decline.
Empirical studies of cognitive aging are often difficult, and quite technical, given their nature. Similarly, experiments focused on one kind of task may tell you very little in terms of general capacities. Memory and attention as psychological constructs are now divided into very specific subsets which can be confusing and difficult to compare.
However, one study does show with relative clarity the issues involved. In the USA, The Federal Aviation Authority insists that all air traffic controllers retire at 56 and that they cannot begin until age 31 unless they have previous military experience. However, in Canada controllers are allowed to work until age 65 and are allowed to train at a much earlier age. Nunes and Kramer (2009) studied four groups: a younger group of controllers (20-27), an older group of controllers aged 53 to 64, and two other groups of the same age who were not air traffic controllers.

On simple cognitive tasks, not related to their occupational lives as controllers, older controllers were slower than their younger peers. However, when it came to job-related tasks their results were largely identical. This was not true of the older group of non-controllers who had significant deficits in comparison. Specific knowledge or expertise in a domain acquired over time (crystallized intelligence), can offset a decline in fluid intelligence.
Tacit Knowledge
The idea of tacit knowledge was first introduced by Michael Polanyi (1954). He argued that each individual had a huge store of knowledge based on life experience, but that it was often difficult to describe, codify, and thus transfer, as stated in his famous formulation, “we always know more than we can tell.” Organizational theorists have spent a great deal of time thinking about the problem of tacit knowledge in this setting. Think of someone you have encountered who is extremely good at what they do. They may have no more (or less) education, formal training, and even experience, than others who are supposedly at an equivalent level. What is the “something” that they have? Tacit knowledge is highly prized and older workers often have the greatest amount, even if they are not conscious of that fact.
Expertise Model
Expertise refers to specialized skills and knowledge that pertain to a particular topic or activity. In contrast, a novice is someone who has limited experiences with a particular task. People often are able to develop a type of expertise in things that they find important. This can be anything from sewing to diagnosing illnesses to making bread. The four main characteristics of expert thought are:
- Intuitive: Because experts have practice, past experience, and knowledge of their craft, they are able to perform their craft without having to follow strict, step-by-step instructions like a novice might have to. This means that experts are less formulaic and more intuitive with their work.
- Automatic: Experts are able to perform their actions in a more instinctive fashion. Even complex thoughts and actions have become routine for experts over time because they can process information faster and more effectively.
- Strategic: The strategies used by experts are more effective than those used by novices. An example of this is how more experienced note-takers can be more efficient at taking notes than a novice at academic note-taking. The expert knows that they do not have to write down every word the instructor says and might even have their own shorthand for often used words, whereas a novice note-taker might waste more time on those things.
- Flexible: Because experts are comfortable with the basics of their craft, they are more likely to be curious, creative, and experiment with new ideas and procedures. By making their actions more challenging than the basic, routine tasks of the novice, experts are able to grow their knowledge even further.
It takes time to gather enough experience and practice to be considered an expert in anything. By the time we hit middle adulthood, we have gained a large store of knowledge and experience. This means that when we face a problem at this point in our lives, it is likely that we have faced something similar before. Because of this, we are able to focus more fully on the important aspects of the issue and be more effiecient in solving it. We tend to gain some sorts of expertise by middle adulthood, which is why many people often reach the top of their career in this developmental stage.
Psychosocial Development in Midlife
What do you think is the happiest stage of life? What about the saddest stages? Perhaps surprisingly, Blanchflower & Oswald (2008) found that reported levels of unhappiness and depressive symptoms peak in the early 50s for men in the U.S., and interestingly, the late 30s for women. In Western Europe, minimum happiness is reported around the mid-40s for both men and women, albeit with some significant national differences. Stone, Schneider and Bradoch (2017), reported a precipitous drop in perceived stress in men in the U.S. from their early 50s.

There is now a view that “older people” (50+) may be “happier” than younger people, despite some cognitive and functional losses. This is often referred to as “the paradox of aging.” Positive attitudes to the continuance of cognitive and behavioral activities, interpersonal engagement, and their vitalizing effect on human neural plasticity, may lead not only to more life, but to an extended period of both self-satisfaction and continued communal engagement.
Erikson’s Theory
As you know by now, Erikson’s theory is based on an idea called epigenesis, meaning that development is progressive and that each individual must pass through the eight different stages of life—all while being influenced by context and environment. Each stage forms the basis for the following stage, and each transition to the next is marked by a crisis which must be resolved. The sense of self, each “season”, was wrested, from and by, that conflict. The ages 40-65 are no different. The individual is still driven to engage productively, but the nurturing of children and income generation assume lesser functional importance. From where will the individual derive their sense of self and self-worth?
Generativity versus Stagnation is Erikson’s characterization of the fundamental conflict of adulthood. It is the seventh conflict of his famous “8 seasons of man” (1950) and negotiating this conflict results in the virtue of care. Generativity is “primarily the concern in establishing and guiding the next generation” (Erikson, 1950 p.267). Generativity is a concern for a generalized other (as well as those close to an individual) and occurs when a person can shift their energy to care for and mentor the next generation. One obvious motive for this generative thinking might be parenthood, but others have suggested intimations of mortality by the self. John Kotre (1984) theorized that generativity is a selfish act, stating that its fundamental task was to outlive the self.

He viewed generativity as a form of investment. However, a commitment to a “belief in the species” can be taken in numerous directions, and it is probably correct to say that most modern treatments of generativity treat it as collection of facets or aspects—encompassing creativity, productivity, commitment, interpersonal care, and so on. On the other side of generativity is stagnation. It is the feeling of lethargy and a lack of enthusiasm and involvement in both individual and communal affairs. It may also denote an underdeveloped sense of self, or some form of overblown narcissism. Erikson sometimes used the word “rejectivity” when referring to severe stagnation.
WATCH THIS video below or online with captions for more information on the stage of Generativity vs Stagnation:
The Stage-Crisis View and the Midlife Crisis
In 1977, Daniel Levinson published an extremely influential article that would be seminal in establishing the idea of a profound crisis which lies at the heart of middle adulthood. The concept of a midlife crisis is so pervasive that over 90% of Americans are familiar with the term, although those who actually report experiencing such a crisis is significantly lower (Wethington, 2000).
Levinson based his findings about a midlife crisis on biographical interviews with a limited sample of 40 men (no women!), and an entirely American sample at that. Despite these severe methodological limitations, his findings proved immensely influential. Levinson (1986) identified five main stages or “seasons” of a man’s life as follows:
- Preadulthood: Ages 0-22 (with 17 – 22 being the Early Adult Transition years)
- Early Adulthood: Ages 17-45 (with 40 – 45 being the Midlife Transition years)
- Middle Adulthood: Ages 40-65 (with 60-65 being the Late Adult Transition years)
- Late Adulthood: Ages 60-85
- Late Late Adulthood: Ages 85+
Levinson’s theory is known as the stage-crisis view. He argued that each stage overlaps, consisting of two distinct phases—a stable phase, and a transitional phase into the following period. The latter phase can involve questioning and change, and Levinson believed that 40-45 was a period of profound change, which could only culminate in a reappraisal, or perhaps reaffirmation, of goals, commitments and previous choices—a time for taking stock and recalibrating what was important in life. Crucially, Levinson would argue that a much wider range of factors, involving, primarily, work and family, would affect this taking stock – what he had achieved, what he had not; what he thought important, but had brought only a limited satisfaction.

In 1996, two years after his death, the study he was conducting with his co-author and wife Judy Levinson, was published on “the seasons of life” as experienced by women. Again, it was a small-scale study, with 45 women who were professionals / businesswomen, academics, and homemakers, in equal proportion. The changing place of women in society was reckoned by Levinson to be a profound moment in the social evolution of the human species, however, it had led to a fundamental polarity in the way that women formed and understood their social identity. Levinson referred to this as the “dream.” For men, the “dream” was formed in the age period of 22-28, and largely centered on the occupational role and professional ambitions. Levinson understood the female “dream” as fundamentally split between this work-centered orientation, and the desire/imperative of marriage/family; a polarity which heralded both new opportunities, and fundamental angst.

Levinson found that the men and women he interviewed sometimes had difficulty reconciling the “dream” they held about the future with the reality they currently experienced. “What do I really get from and give to my wife, children, friends, work, community-and self?” a man might ask (Levinson, 1978, p. 192). Tasks of the midlife transition include:
- ending early adulthood;
- reassessing life in the present and making modifications if needed; and
- reconciling “polarities” or contradictions in ones sense of self.
Perhaps early adulthood ends when a person no longer seeks adult status but feels like a full adult in the eyes of others. This “permission” may lead to different choices in life—choices that are made for self-fulfillment instead of social acceptance. While people in their 20s may emphasize how old they are (to gain respect, to be viewed as experienced), by the time people reach their 40s, they tend to emphasize how young they are (few 40 year-olds cut each other down for being so young: “You’re only 43? I’m 48!!”).
This new perspective on time brings about a new sense of urgency to life. The person becomes focused more on the present than the future or the past. The person grows impatient at being in the “waiting room of life,” postponing doing the things they have always wanted to do. “If it’s ever going to happen, it better happen now.” A previous focus on the future gives way to an emphasis on the present. Neugarten (1968) notes that in midlife, people no longer think of their lives in terms of how long they have lived. Rather, life is thought of in terms of how many years are left. If an adult is not satisfied at midlife, there is a new sense of urgency to start to make changes now.
Changes may involve ending a relationship or modifying one’s expectations of a partner. These modifications are easier than changing the self (Levinson, 1978). Midlife is a period of transition in which one holds earlier images of the self while forming new ideas about the self of the future. A greater awareness of aging accompanies feelings of youth, and harm that may have been done previously in relationships haunts new dreams of contributing to the well-being of others. These polarities are the quieter struggles that continue after outward signs of “crisis” have gone away.
Levinson characterized midlife as a time of developmental crisis. However, like any body of work, it has been subject to criticism. Firstly, the sample size of the populations on which he based his primary findings is too small. By what right do we generalize findings from interviews with 40 men, and 45 women, however thoughtful and well conducted? Secondly, Chiriboga (1989) could not find any substantial evidence of a midlife crisis, and it might be argued that this, and further failed attempts at replication, indicate a cohort effect. The findings from Levinson’s population indicated a shared historical and cultural situatedness, rather than a cross-cultural universal experienced by all or even most individuals. Midlife is a time of revaluation and change, that may escape precise determination in both time and geographical space, but people do emerge from it, and seem to enjoy a period of contentment, reconciliation and acceptance of self.
WATCH THIS video below or online explaining research and controversy surrounding the concept of a midlife crisis:
Socio-Emotional Selectivity Theory (SST)
It is the inescapable fate of human beings to know that their lives are limited. As people move through life, goals and values tend to shift. What we consider priorities, goals, and aspirations are subject to renegotiation. Attachments to others, current and future, are no different. Time is not the unlimited good as perceived by a child under normal social circumstances; it is very much a valuable commodity, requiring careful consideration in terms of the investment of resources. This has become known in the academic literature as mortality salience.
Mortality salience posits that reminders about death or finitude (at either a conscious or subconscious level), fills us with dread. We seek to deny its reality, but awareness of the increasing nearness of death can have a potent effect on human judgement and behavior. This has become a very important concept in contemporary social science. It is with this understanding that Laura Carstensen developed the theory of socioemotional selectivity theory, or SST. The theory maintains that as time horizons shrink, as they typically do with age, people become increasingly selective, investing greater resources in emotionally meaningful goals and activities. According to the theory, motivational shifts also influence cognitive processing. Aging is associated with a relative preference for positive over negative information. This selective narrowing of social interaction maximizes positive emotional experiences and minimizes emotional risks as individuals become older. They systematically hone their social networks so that available social partners satisfy their emotional needs. An adaptive way of maintaining a positive affect might be to reduce contact with those we know may negatively affect us, and avoid those who might.
SST is a theory which emphasizes a time perspective rather than chronological age. When people perceive their future as open ended, they tend to focus on future-oriented development or knowledge-related goals. When they feel that time is running out, and the opportunity to reap rewards from future-oriented goals’ realization is dwindling, their focus tends to shift towards present-oriented and emotion or pleasure-related goals. Research on this theory often compares age groups (e.g., young adulthood vs. old adulthood), but the shift in goal priorities is a gradual process that begins in early adulthood. Importantly, the theory contends that the cause of these goal shifts is not age itself, i.e., not the passage of time itself, but rather an age-associated shift in time perspective. The theory also focuses on the types of goals that individuals are motivated to achieve. Knowledge-related goals aim at knowledge acquisition, career planning, the development of new social relationships and other endeavors that will pay off in the future. Emotion-related goals are aimed at emotion regulation, the pursuit of emotionally gratifying interactions with social partners, and other pursuits whose benefits which can be realized in the present.
This shift in emphasis, from long term goals to short term emotional satisfaction, may help explain the previously noted “paradox of aging.” That is, that despite noticeable physiological declines, and some notable self-reports of reduced life-satisfaction around this time, post- 50 there seems to be a significant increase in reported subjective well-being. SST does not champion social isolation, which is harmful to human health, but shows that increased selectivity in human relationships, rather than abstinence, leads to more positive affect. Perhaps “midlife crisis and recovery” may be a more apt description of the 40-65 period of the lifespan.
WATCH THIS TEDx talk below or online with captions by Laura Carstensen explaining how happiness actually increases with age:
Selection, Optimization, Compensation (SOC)
Another perspective on aging was identified by German developmental psychologists Paul and Margret Baltes. Their text Successful Aging marked a seismic shift in moving social science research on aging from largely a deficits-based perspective to a newer understanding based on a holistic view of the life-course itself. The former had tended to focus exclusively on what was lost during the aging process, rather than seeing it as a balance between those losses and gains in areas like the regulation of emotion, experience and wisdom. The Baltes’ model for successful aging argues that across the lifespan, people face various opportunities or challenges such as, jobs, educational opportunities, and illnesses. According to the SOC model, a person may select particular goals or experiences, or circumstances might impose themselves on them. Either way, the selection process includes shifting or modifying goals based on choice or circumstance in response to those circumstances. The change in direction may occur at the subconscious level. This model emphasizes that setting goals and directing efforts towards a specific purpose is beneficial to healthy aging. Optimization is about making the best use of the resources we have in pursuing goals. Compensation, as its name suggests, is about using alternative strategies in attaining those goals.

The processes of selection, optimization, and compensation can be found throughout the lifespan. As we progress in years, we select areas in which we place resources, hoping that this selection will optimize the resources that we have, and compensate for any defects accruing from physiological or cognitive changes. Previous accounts of aging had understated the degree to which possibilities from which we choose had been eliminated, rather than reduced, or even just changed. As we select areas in which to invest, there is always an opportunity cost. We are masters of our own destiny, and our own individual orientation to the SOC processes will dictate “successful aging.” Rather than seeing aging as a process of progressive disengagement from social and communal roles undertaken by a group, Baltes argued that “successful aging” was a matter of sustained individual engagement, accompanied by a belief in individual self-efficacy and mastery.
The SOC model covers a number of functional domains—motivation, emotion, and cognition. We might become more adept at playing the SOC game as time moves on, as we work to compensate and adjust for changing abilities across the lifespan. For example, a soccer a player at 35 may no longer have the vascular and muscular fitness that they had at 20 but her “reading” of the game might compensate for this decline. She may well be a better player than she was at 20, even with fewer physical resources in a game which ostensibly prioritizes them. The work of Paul and Margaret Baltes was very influential in the formation of a very broad developmental perspective which would coalesce around the central idea of resiliency.
Personality and Work Satisfaction
The Five Factor Model
Research on adult personality examines normative age-related increases and decreases in the expression of the so-called “Big Five” traits—extroversion, neuroticism, conscientiousness, agreeableness, and openness to experience. These are assumed to be based largely on biological heredity. These five traits are sometimes summarized via the OCEAN acronym. Individuals are assessed by the measurement of these traits along a continuum (e.g. high extroversion to low extroversion). They now dominate the field of empirical personality research. Does personality change throughout adulthood? Previously the answer was thought to be no. It was William James who stated in his foundational text, The Principles of Psychology (1890), that “[i]n most of us, by the age of thirty, the character is set like plaster, and will never soften again”. Not surprisingly, this became known as the plaster hypothesis.
In the Five Factor Model, each person has each factor, but they occur along a spectrum:
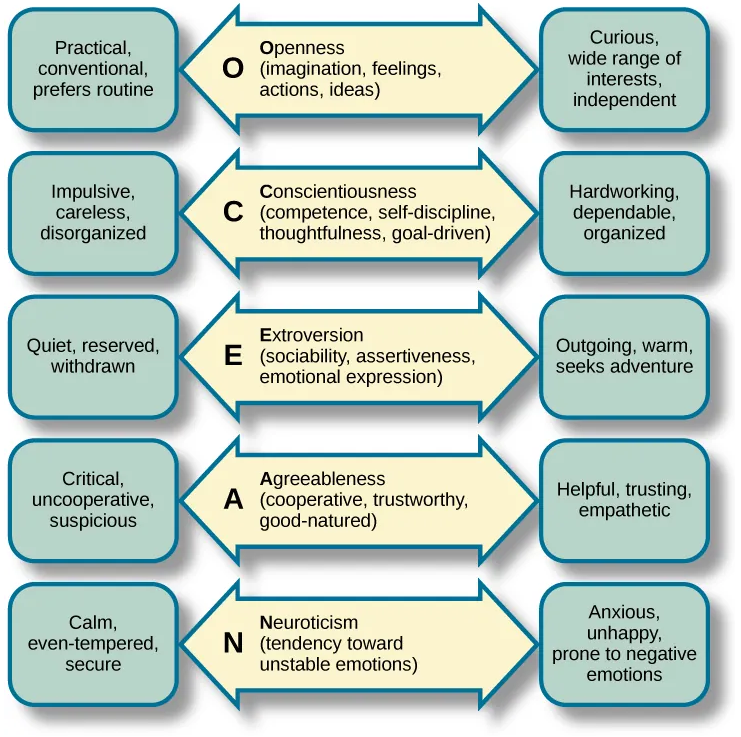
Openness to experience is characterized by imagination, feelings, actions, and ideas. People who score high on this factor tend to be curious and have a wide range of interests. Conscientiousness is characterized by competence, self-discipline, thoughtfulness, and achievement-striving (goal-directed behavior). People who score high on this factor are hardworking and dependable. Numerous studies have found a positive correlation between conscientiousness and academic success. Extroversion is characterized by sociability, assertiveness, excitement-seeking, and emotional expression. People who score high on this factor are usually described as outgoing and warm. Not surprisingly, people who score high on both extroversion and openness are more likely to participate in adventure and risky sports due to their curious and excitement-seeking nature. The fourth factor is agreeableness, which is the tendency to be pleasant, cooperative, trustworthy, and good-natured.
People who score low on agreeableness tend to be described as rude and uncooperative, yet one recent study reported that men who scored low on this factor actually earned more money than men who were considered more agreeable. The last of the Big Five factors is neuroticism, which is the tendency to experience negative emotions. People high on neuroticism tend to experience emotional instability and are characterized as angry, impulsive, and hostile. Watson and Clark (1984) found that people reporting high levels of neuroticism also tend to report feeling anxious and unhappy. In contrast, people who score low in neuroticism tend to be calm and even-tempered.
Contemporary research shows that, although some people’s personalities are relatively stable over time, others’ are not (Lucas & Donnellan, 2011; Roberts & Mroczek, 2008). Longitudinal studies reveal average changes during adulthood, and individual differences in these patterns over the lifespan may be due to idiosyncratic life events (e.g., divorce, illness). Roberts, Wood & Caspi (2008) report evidence of increases in agreeableness and conscientiousness as persons age, mixed results in regard to openness, reduction in neuroticism but only in women, and no change with regard to extroversion. Whether this “maturation” is the cause or effect of some of the changes noted in the section devoted to psycho social development is still unresolved. Longitudinal research also suggests that adult personality traits, such as conscientiousness, predict important life outcomes including job success, health, and longevity (Friedman, Tucker, Tomlinson-Keasey, Schwartz, Wingard, & Criqui, 1993; Roberts, Kuncel, Shiner, Caspi, & Goldberg, 2007). How important these changes are remains somewhat unresolved. Thus, we have the hard plaster hypothesis, emphasizing fixity in personality over the age of thirty with some very minor variation, and the soft plaster version which views these changes as possible and important.
Carl Jung believed that our personality actually matures as we get older. A healthy personality is one that is balanced. People suffer tension and anxiety when they fail to express all of their inherent qualities. Jung believed that each of us possess a “shadow side.” For example, those who are typically introverted also have an extroverted side that rarely finds expression unless we are relaxed and uninhibited. Each of us has both a masculine and feminine side, but in younger years, we feel societal pressure to give expression only to one. As we get older, we may become freer to express all of our traits as the situation arises. We find gender convergence in older adults. Men become more interested in intimacy and family ties. Women may become more assertive. This gender convergence is also affected by changes in society’s expectations for males and females. With each new generation we find that the roles of men and women are less stereotypical, and this allows for change as well.

Subjective Aging
One aspect of the self that particularly interests life span and life course psychologists is the individual’s perception and evaluation of their own aging and identification with an age group. Subjective age is a multidimensional construct that indicates how old (or young) a person feels, and into which age group a person categorizes themself. After early adulthood, most people say that they feel younger than their chronological age, and the gap between subjective age and actual age generally increases. On average, after age 40 people report feeling 20% younger than their actual age (e.g., Rubin & Berntsen, 2006). Asking people how satisfied they are with their own aging assesses an evaluative component of age identity. Whereas some aspects of age identity are positively valued (e.g., acquiring seniority in a profession or becoming a grandparent), others may be less valued, depending on societal context. Perceived physical age (i.e., the age one looks in a mirror) is one aspect that requires considerable self-related adaptation in social and cultural contexts that value young bodies. Feeling younger and being satisfied with one’s own aging are expressions of positive self-perceptions of aging. They reflect the operation of self-related processes that enhance well-being. Levy (2009) found that older individuals who are able to adapt to and accept changes in their appearance and physical capacity in a positive way report higher well-being, have better health, and live longer.
There is now an increasing acceptance of the view within developmental psychology that an uncritical reliance on chronological age may be inappropriate. People have certain expectations about getting older, their own idiosyncratic views, and internalized societal beliefs. Taken together they constitute a tacit knowledge of the aging process. A negative perception of how we are aging can have real results in terms of life expectancy and poor health. Levy et al (2002) estimated that those with positive feelings about aging lived 7.5 years longer than those who did not. Subjective aging encompasses a wide range of psychological perspectives and empirical research. However, there is now a growing body of work centered around a construct referred to as Awareness of Age Related Change (AARC) (Diehl et al, 2015), which examines the effects of our subjective perceptions of age and their consequential, and very real, effects. Neuport & Bellingtier (2017) report that this subjective awareness can change on a daily basis, and that negative events or comments can disproportionately affect those with the most positive outlook on aging.
Work Satisfaction
Middle adulthood is characterized by a time of transition, change, and renewal. Accordingly, attitudes about work and satisfaction from work tend to undergo a transformation or reorientation during this time. Age is positively related to job satisfaction—the older we get the more we derive satisfaction from work (Ng & Feldman, 2010). However, that is far from the entire story and repeats, once more, the paradoxical nature of the research findings from this period of the life course. Dobrow, Gazach & Liu (2018) found that job satisfaction in those aged 43-51 was correlated with advancing age, but that there was increased dissatisfaction the longer one stayed in the same job. Again, as socio-emotional selectivity theory would predict, there is a marked reluctance to tolerate a work situation deemed unsuitable or unsatisfying. Years left, as opposed to years spent, necessitates a sense of purpose in all daily activities and interactions, including work
The workplace today is one in which many people from various walks of life come together. Work schedules are more flexible and varied, and more work independently from home or anywhere there is an internet connection. The midlife worker must be flexible, stay current with technology, and be capable of working within a global community.
Relationships at Work
Working adults spend a large part of their waking hours in relationships with coworkers and supervisors. Because these relationships are forced upon us by work, researchers focus less on their presence or absence and instead focus on their quality. High quality work relationships can make jobs enjoyable and less stressful. This is because workers experience mutual trust and support in the workplace to overcome work challenges. Liking the people we work with can also translate to more humor and fun on the job. Research has shown that supervisors who are more supportive have employees who are more likely to thrive at work (Paterson, Luthans, & Jeung, 2014; Monnot & Beehr, 2014; Winkler, Busch, Clasen, & Vowinkel, 2015).

On the other hand, poor quality work relationships can make a job feel like drudgery. Everyone knows that horrible bosses can make the workday unpleasant. Supervisors that are sources of stress have a negative impact on the subjective well-being of their employees (Monnot & Beehr, 2014).
Specifically, research has shown that employees who rate their supervisors high on the so-called “dark triad”—psychopathy, narcissism, and Machiavellianism—reported greater psychological distress at work, as well as less job satisfaction (Mathieu, Neumann, Hare, & Babiak, 2014).
In addition to the direct benefits or costs of work relationships on our well-being, we should also consider how these relationships can impact our job performance. Research has shown that feeling engaged in our work and having a high job performance predicts better health and greater life satisfaction (Shimazu, Schaufeli, Kamiyama, & Kawakami, 2015). Given that so many of our waking hours are spent on the job—about 90,000 hours across a lifetime—it makes sense that we should seek out and invest in positive relationships at work.
One of the most influential researchers in this field, Dorien Kooij (2013) identified four key motivations in older adults continuing to work. First, growth or development motivation- looking for new challenges in the work environment. The second are feelings of recognition and power. Third, feelings of power and security afforded by income and possible health benefits. Interestingly enough, the fourth area of motivation was Erikson’s generativity. The latter has been criticized for a lack of support in terms of empirical research findings, but two studies (Zacher et al, 2012; Ghislieri & Gatti, 2012) found that a primary motivation in continuing to work was the desire to pass on skills and experience, a process they describe as leader generativity. Perhaps a more straightforward term might be mentoring. In any case, the concept of generative leadership is now firmly established in the business and organizational management literature.
Organizations, public and private, are going to have to deal with an older workforce. The proportion of people in Europe over 60 will increase from 24% to 34% by 2050 (United Nations 2015), the US Bureau of Labor Statistics predicts that 1 in 4 of the US workforce will be 55 or over. Workers may have good reason to avoid retirement, although it is often viewed as a time of relaxation and well-earned rest, statistics may indicate that a continued focus on the future may be preferable to stasis, or inactivity. In fact, Fitzpatrick & Moore (2018) report that death rates for American males jump 2% immediately after they turn 62, most likely a result of changes induced by retirement. Interestingly, this small spike in death rates is not seen in women, which may be the result of women having stronger social determinants of health (SDOH), which keep them active and interacting with others out of retirement.
Relationships & Family Life in Middle Adulthood
Types of Relationships
Intimate Relationships
It makes sense to consider the various types of relationships in our lives when trying to determine just how relationships impact our well-being. For example, would you expect a person to derive the same happiness from an ex-spouse as from a child or coworker? Among the most important relationships for most people is their long-time romantic partner. Most researchers begin their investigation of this topic by focusing on intimate relationships because they are the closest form of social bond. Intimacy is more than just physical in nature; it also entails psychological closeness. Research findings suggest that having a single confidante—a person with whom you can be authentic and trust not to exploit your secrets and vulnerabilities—is more important to happiness than having a large social network (Taylor, 2010).

Another important aspect is the distinction between formal and informal relationships. Formal relationships are those that are bound by the rules of politeness. In most cultures, for instance, young people treat older people with formal respect by avoiding profanity and slang when interacting with them. Similarly, workplace relationships tend to be more formal, as do relationships with new acquaintances. Formal connections are generally less relaxed because they require a bit more work, demanding that we exert more self-control. Contrast these connections with informal relationships—friends, lovers, siblings, or others with whom you can relax. We can express our true feelings and opinions in these informal relationships, using the language that comes most naturally to us, and generally be more authentic. Because of this, it makes sense that more intimate relationships—those that are more comfortable and in which you can be more vulnerable—might be the most likely to translate to happiness.
Marriage and Happiness
One of the most common ways that researchers often begin to investigate intimacy is by looking at marital status. The well-being of married people is compared to that of people who are single or have never been married. In other research, married people are compared to people who are divorced or widowed (Lucas & Dyrenforth, 2005). Researchers have found that the transition from singlehood to marriage brings about an increase in subjective well-being (Haring-Hidore, Stock, Okun, & Witter, 1985; Lucas, 2005; Williams, 2003). In fact, this finding is one of the strongest in social science research on personal relationships over the past quarter of a century.

As is usually the case, the situation is more complex than might initially appear. As a marriage progresses, there is some evidence for a regression to a hedonic set-point—that is, most individuals have a set happiness point or level, and that both good and bad life events – marriage, bereavement, unemployment, births and so on – have some effect for a period of time, but over many months, they will return to that set-point. One of the best studies in this area is that of Luhmann et al (2012), who report a gradual decline in subjective well-being after a few years, especially in the component of affective well-being. Adverse events obviously have an effect on subjective well-being and happiness, and these effects can be stronger than the positive effects of being married in some cases (Lucas, 2005).
WATCH THIS video below or online explaining why better circumstances doesn’t always mean we are happier:
Although research frequently points to marriage being associated with higher rates of happiness, this does not guarantee that getting married will make you happy! The quality of one’s marriage matters greatly. When a person remains in a problematic marriage, it takes an emotional toll. Indeed, a large body of research shows that people’s overall life satisfaction is affected by their satisfaction with their marriage. The lower a person’s self-reported level of marital quality, the more likely they are to report depression. In fact, longitudinal studies—those that follow the same people over a period of time—show that as marital quality declines, depressive symptoms increase. Proulx and colleagues (2007) arrived at this same conclusion after a systematic review of 66 cross-sectional and 27 longitudinal studies.
Although research frequently points to marriage being associated with higher rates of happiness, this does not guarantee that getting married will make you happy! The quality of one’s marriage matters greatly. When a person remains in a problematic marriage, it takes an emotional toll. Indeed, a large body of research shows that people’s overall life satisfaction is affected by their satisfaction with their marriage (Carr, Freedman, Cornman, Schwarz, 2014; Dush, Taylor, & Kroeger, 2008; Karney, 2001; Luhmann, Hofmann, Eid, & Lucas, 2012; Proulx, Helms, & Buehler, 2007). The lower a person’s self-reported level of marital quality, the more likely he or she is to report depression (Bookwala, 2012). In fact, longitudinal studies—those that follow the same people over a period of time—show that as marital quality declines, depressive symptoms increase (Fincham, Beach, Harold, & Osborne, 1997; Karney, 2001). Proulx and colleagues (2007) arrived at this same conclusion after a systematic review of 66 cross-sectional and 27 longitudinal studies.
Marital satisfaction has peaks and valleys during the course of the life cycle. Rates of happiness are highest in the years prior to the birth of the first child. It hits a low point with the coming of children. Relationships typically become more traditional and there are more financial hardships and stress in living. Children bring new expectations to the marital relationship. Two people who are comfortable with their roles as partners may find the added parental duties and expectations more challenging to meet. Some couples elect not to have children in order to have more time and resources for the marriage. These child-free couples are happy keeping their time and attention on their partners, careers, and interests.

What is it about bad marriages, or bad relationships in general, that takes such a toll on well-being? Research has pointed to conflict between partners as a major factor leading to lower subjective well-being (Gere & Schimmack, 2011). This makes sense. Negative relationships are linked to ineffective social support (Reblin, Uchino, & Smith, 2010) and are a source of stress (Holt-Lunstad, Uchino, Smith, & Hicks, 2007). In more extreme cases, physical and psychological abuse can be detrimental to well-being (Follingstad, Rutledge, Berg, Hause, & Polek, 1990). Victims of abuse sometimes feel shame, lose their sense of self, and become less happy and prone to depression and anxiety (Arias & Pape, 1999). However, the unhappiness and dissatisfaction that occur in abusive relationships tend to dissipate once the relationships end. (Arriaga, Capezza, Goodfriend, Rayl & Sands, 2013).
WATCH THIS video below or online with captions to learn more on the Family Life Cycle:
Marital Communication
Advice on how to improve one’s marriage is centuries old. One of today’s experts on marital communication is John Gottman. Gottman differs from many marriage counselors in his belief that having a good marriage does not depend on compatibility, rather, the way that partners communicate with one another is crucial. At the University of Washington in Seattle, Gottman has measured the physiological responses of thousands of couples as they discuss issues which have led to disagreements. Fidgeting in one’s chair, leaning closer to or further away from the partner while speaking, and increases in respiration and heart rate are all recorded and analyzed, along with videotaped recordings of the partners’ exchanges.
WATCH THIS video below or online with captions explaining Gottman’s ideas on “repair attempts” in relationships:
Gottman believes he can accurately predict whether or not a couple will stay together by analyzing their communication. In marriages destined to fail, partners engage in the “marriage killers” such as contempt, criticism, defensiveness, and stonewalling. Each of these undermines the politeness and respect that healthy marriages require. According to Gottman, stonewalling, or shutting someone out, is the strongest sign that a relationship is destined to fail. Perhaps the most interesting aspect of Gottman’s work is the emphasis on the fact that marriage is about constant negotiation rather than conflict resolution.
What Gottman terms perpetual problems, are responsible for 69% of conflicts within marriage. For example, if someone in a couple has said, “I am so sick of arguing over this,” then that may be a sign of perpetual problem. While this may seem problematic, Gottman argues that couples can still be connected despite these perpetual problems if they can laugh about it, treat it as a “third thing” (not reducible to the perspective of either party), and recognize that these are part of relationships that need to be aired and dealt with as best you can. It is somewhat refreshing to hear that differences lie at the heart of marriage, rather than a rationale for its dissolution!

Parenting in Later Life
Just because children grow up does not mean their family stops being a family, rather the specific roles and expectations of its members change over time. One major change comes when a child reaches adulthood and moves away. When exactly children leave home varies greatly depending on societal norms and expectations, as well as on economic conditions such as employment opportunities and affordable housing options. Some parents may experience sadness when their adult children leave the home—a situation called an empty nest.
Many parents are also finding that their grown children are struggling to launch into independence. It’s an increasingly common story: a child goes off to college and, upon graduation, is unable to find steady employment. In such instances, a frequent outcome is for the child to return home, becoming a “boomerang kid.” The boomerang generation, as the phenomenon has come to be known, refers to young adults, mostly between the ages of 25 and 34, who return home to live with their parents while they strive for stability in their lives—often in terms of finances, living arrangements, and sometimes romantic relationships. These boomerang kids can be both good and bad for families. Within American families, 48% of boomerang kids report having paid rent to their parents, and 89% say they help out with household expenses—a win for everyone (Parker, 2012). On the other hand, 24% of boomerang kids report that returning home hurts their relationship with their parents (Parker, 2012). For better or for worse, the number of children returning home has been increasing around the world. The Pew Research Center (2016) reported that the most common living arrangement for people aged 18-34 was living with their parents (32.1%).
Adult children typically maintain frequent contact with their parents, if for no other reason, money and advice. Attitudes toward one’s parents may become more accepting and forgiving, as parents are seen in a more objective way, as people with good points and bad. As adults, children can continue to be subjected to criticism, ridicule, and abuse at the hand of parents. How long are we “adult children”? For as long as our parents are living, we continue in the role of son or daughter. (I had a neighbor in her nineties who would tell me her “boys” were coming to see her this weekend. Her boys were in their 70s-but they were still her boys!) But after one’s parents are gone, the adult is no longer a child; as one 40-year-old man explained after the death of his father, “I’ll never be a kid again.”
Family Issues and Considerations
In addition to middle-aged parents spending more time, money, and energy taking care of their adult children, they are also increasingly taking care of their own aging and ailing parents. Middle-aged people in this set of circumstances are commonly referred to as the sandwich generation (Dukhovnov & Zagheni, 2015). Of course, cultural norms and practices again come into play. In some Asian and Hispanic cultures, the expectation is that adult children are supposed to take care of aging parents and parents-in-law. In other Western cultures—cultures that emphasize individuality and self-sustainability—the expectation has historically been that elders either age in place, modifying their home and receiving services to allow them to continue to live independently, or enter long-term care facilities. However, given financial constraints, many families find themselves taking in and caring for their aging parents, increasing the number of multigenerational homes around the world.


Being a midlife child often involves kinkeeping; organizing events and communication in order to maintain family ties. This role was first defined by Carolyn Rosenthal (1985). Kinkeepers are often midlife daughters (they are the person who tells you what food to bring to a gathering, or makes arrangement for a family reunion). They can often function as “managers” who maintain family ties and lines of communication. This is true for both large nuclear families, reconstituted, and multi-generational families. Rosenthal found that over half of the families she sampled were capable of identifying the individual who performed this role. Often adults at this stage of their lives are pressed into caregiving roles. Often referred to as the “sandwich generation”, they are still looking out for their own children while simultaneously caring for elderly parents. Given shifts in longevity and increasing costs for professional care of the elderly, this role will likely expand, placing ever greater pressure on careers.
Abuse in Family Life
Abuse can occur in multiple forms and across all family relationships. Breiding, Basile, Smith, Black, & Mahendra (2015) define the forms of abuse as:
Physical abuse: the use of intentional physical force to cause harm. Scratching, pushing, shoving, throwing, grabbing, biting, choking, shaking, slapping, punching, and hitting are common forms of physical abuse
Sexual abuse: the act of forcing someone to participate in a sex act against their will. Such abuse is often referred to as sexual assault or rape. A marital relationship does not grant anyone the right to demand sex or sexual activity from anyone, even a spouse
Psychological abuse: aggressive behavior that is intended to control someone else. Such abuse can include threats of physical or sexual abuse, manipulation, bullying, and stalking.
Abuse between partners is referred to as intimate partner violence; however, such abuse can also occur between a parent and child (child abuse), adult children and their aging parents (called Elder Abuse), and even between siblings.
The most common form of abuse between parents and children is that of neglect. Neglect refers to a family’s failure to provide for a child’s basic physical, emotional, medical, or educational needs (DePanfilis, 2006). Harry Potter’s aunt and uncle, as well as Cinderella’s stepmother, could all be prosecuted for neglect in the real world.
Abuse is a complex issue, especially within families. There are many reasons people become abusers: poverty, stress, and substance abuse are common characteristics shared by abusers, although abuse can happen in any family. There are also many reasons adults stay in abusive relationships: (a) learned helplessness (the abused person believing he or she has no control over the situation); (b) the belief that the abuser can/will change; (c) shame, guilt, self-blame, and/or fear; and (d) economic dependence. All of these factors can play a role.
Children who experience abuse may “act out” or otherwise respond in a variety of unhealthy ways. These include acts of self-destruction, withdrawal, and aggression, as well as struggles with depression, anxiety, and academic performance. Researchers have found that abused children’s brains may produce higher levels of stress hormones. These hormones can lead to decreased brain development, lower stress thresholds, suppressed immune responses, and lifelong difficulties with learning and memory (Middlebrooks & Audage, 2008).
CLICK OR CALL THESE resources to get help and support for stopping or recovering from abuse: The Child Help Hotline provides confidential support and guidance for teens and adults who are experiencing, have experienced, are witnessing or have witnessed any type of child abuse. They support people who are unsure how to report or support victims as well as people looking for resources to cope with past abuse. That includes answering questions, providing resources & support, and talking through difficult situations. You can call or text (1-800-422-4453) or chat through their website. RAINN.org is the Rape, Abuse and Incest National Network. They have lots of resources for survivors on their website including the National Sexual Assault Hotline which has chat, phone (1-800-656-HOPE), mobile app, and Chatbot options and will connect you with a trained staff member who can provide confidential crisis support. The National Domestic Violence Support Hotline is a place to start to get confidential resources and support for people experiencing or recovering from Intimate Partner Violence.
Happy Healthy Families
Our families play a crucial role in our overall development and happiness. They can support and validate us, but they can also criticize and burden us. For better or worse, we all have a family. In closing, here are strategies you can use to increase the happiness of your family:
- Teach morality—fostering a sense of moral development in children can promote well-being (Damon, 2004).
- Savor the good—celebrate each other’s successes (Gable, Gonzaga & Strachman, 2006).
- Use the extended family network—family members of all ages, including older siblings and grandparents, who can act as caregivers can promote family well-being (Armstrong, Birnie-Lefcovitch & Ungar, 2005).
- Create family identity—share inside jokes, fond memories, and frame the story of the family (McAdams, 1993).
- Forgive—Don’t hold grudges against one another (McCullough, Worthington & Rachal, 1997).
Divorce and Remarriage
Divorce refers to the legal dissolution of a marriage. Depending on societal factors, divorce may be more or less of an option for married couples. Despite popular belief, divorce rates in the United States actually declined for many years during the 1980s and 1990s, and only just recently started to climb back up—landing at just below 50% of marriages ending in divorce today (Marriage & Divorce, 2016); however, it should be noted that divorce rates increase for each subsequent marriage, and there is considerable debate about the exact divorce rate. Are there specific factors that can predict divorce? Are certain types of people or certain types of relationships more or less at risk for breaking up? Indeed, there are several factors that appear to be either risk factors or protective factors.
Pursuing education decreases the risk of divorce. So too does waiting until we are older to marry. Likewise, if our parents are still married we are less likely to divorce. Factors that increase our risk of divorce include having a child before marriage and living with multiple partners before marriage, known as serial cohabitation (cohabitation with one’s expected marital partner does not appear to have the same effect). Of course, societal and religious attitudes must also be taken into account. In societies that are more accepting of divorce, divorce rates tend to be higher. Likewise, in religions that are less accepting of divorce, divorce rates tend to be lower. See Lyngstad & Jalovaara (2010) for a more thorough discussion of divorce risk.
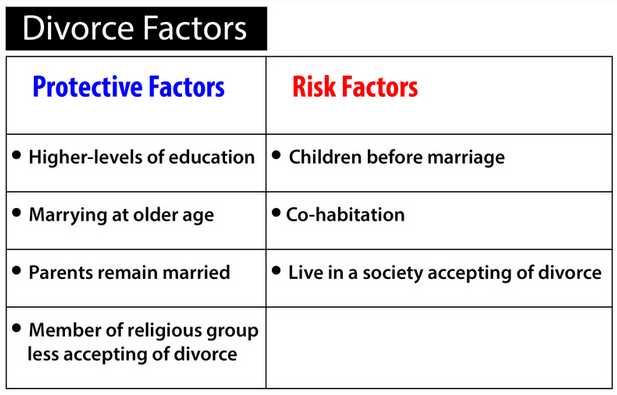
If a couple does divorce, there are specific considerations they should take into account to help their children cope. Parents should reassure their children that both parents will continue to love them and that the divorce is in no way the children’s fault. Parents should also encourage open communication with their children and be careful not to bias them against their “ex” or use them as a means of hurting their “ex” (Denham, 2013; Harvey & Fine, 2004; Pescosoido, 2013).
A “Gray Divorce Revolution”?
In 2013 Brown and Lin referred to a “gray divorce revolution”. The figures certainly seem to support their contention. The rate of divorce had doubled for those aged 50-64 in the twenty years between 1990 and 2010. One in 10 persons who divorced in 1990 was over age 50, by 2010 it was over 1 in 4, accounting for some 25% of all divorces in the USA. Various explanations have been offered for this phenomenon. The “baby boomers” had divorced in large numbers in early adulthood, and a large number of remarriages within this group also ended in divorce. Remarriages are about 2.5 times more likely to end in divorce than first marriages. People are living longer and are no longer satisfied with relationships deemed insufficient to meet their emotional needs. The shift to companionate marriage in the later half of the 20th century had followed this segment of the population into midlife, with divorce rates diminishing or stabilizing for other segments of the population.
Socio-emotional selectivity theory would predict that the shift of perspective from time spent to time remaining would predict people valuing experiences and relationships in the present, rather than holding onto memories of the past, or an idealized vision of what might yet come to be. Nevertheless, Cohen (2018) predicts a substantial decline in divorce rates for those who are not part of the “baby boom” generation, and that marriage rates will stabilize once more in subsequent generational cohorts. There has been a marked decline in divorce rates for those under 45 and the link between college education and marriage is now quite pronounced. People are now waiting until later in life to marry for the first time. The average age is now 27 for women and 29 for men, and it is even higher in urban centers like NYC. However, Reeves et al (2016) show that just over half of women with high school diplomas in their 40s are married, with the figures rising to 75% of those women with Bachelors degrees. Increasing economic insecurity may have played a part in ensuring that marriage may increasingly be correlated with educational attainment and socioeconomic status rather than cohorts based solely on age.
U.S. households are now increasingly single person households. The number is reckoned to be in excess of 28% of all households, and may become the most common form in the near future, if trends in Europe are anything to go by. There, the number of one-person households in countries and Denmark and Germany exceeds 40%, with other major European countries like France not far from reaching that proportion. The number of Americans who are unmarried continues to increases. About 45% of all Americans over the age of 18 are unmarried, in 1960 that number was 28%. Around 1 in 4 young adults in the USA today will never marry. The diversity of households will continue to increase. Currently, the number of one-person households in Japan and Germany is double that of households with children under 18.

Remarriage and Re-partnering
Middle adulthood seems to be the prime time for remarriage, as the Pew Research Center reported in 2014 that of those aged between 55-64 who had previously been divorced, 67% had remarried. In 1960, it was 55%. Every other age category reported declines in the number of remarriages. Notably, remarriage is more popular with men than women, a gender gap that not only persists, but grows substantially in middle and later adulthood. Cohabitation is the main way couples prepare for remarriage, but even when living together, many important issues are still not discussed. Issues concerning money, ex-spouses, children, visitation, future plans, previous difficulties in marriage, etc. can all pose problems later in the relationship. Few couples engage in premarital counseling or other structured efforts to cover this ground before entering into marriage again.
The divorce rate for second marriages is reckoned to be in excess of 60%, and for third marriages even higher. There is little research in the area of repartnering and remarriage, and the choices and decisions made during the process. A notable exception is that of Brown et al (2019) who offer an overview of the little that there is, and their own conclusions. One important constraint which they note is that men prefer younger women, at least as far as remarriage is concerned. Indeed, the gap in age is often more pronounced in second marriages than in the first, according to Pew (2014).

Allied to the fact that women live, on average, five years longer in the USA, then the pool of available partners shrinks for women. Brown et al (2019), also argue that this is further reinforced by the fact that women prefer retaining their autonomy and not playing the role of caregiver again. Perhaps the most interesting aspect of their research is the fact that those who repartner tend to do so quickly, and that longer-term singles are more likely to remain so.
Reviews are mixed as to how happy remarriages are. Some say that they have found the right partner and have learned from mistakes. But the divorce rates for remarriages are higher than for first marriages. This is especially true in stepfamilies for reasons which we have already discussed. People who have remarried tend to divorce more quickly than those first marriages. This may be due to the fact that they have fewer constraints on staying married (are more financially or psychologically independent).
Factors Affecting Remarriage
The chances of remarrying depend on a number of things. First, it depends on the availability of partners. As time goes by, there are more available women than men in the marriage pool as noted above. Consequently, men are more likely than women to remarry. This lack of available partners is experienced by all women, but especially by African-American women where the ratio of women to men is quite high. Women are more likely to have children living with them, and this diminishes the chance of remarriage as well. And marriage is more attractive for males than females (Seccombe & Warner, 2004). Men tend to remarry sooner (3 years after divorce on average vs. 5 years on average for women).
Many women do not remarry because they do not want to remarry. Traditionally, marriage has provided more benefits to men than to women. Women typically have to make more adjustments in work (accommodating work life to meet family demands or the approval of the husband) and at home (taking more responsibility for household duties). Education increases men’s likelihood of remarrying but may reduce the likelihood for women. Part of this is due to the expectation (almost an unspoken rule) referred to as the “marriage gradient.” This rule suggests among couples, the man is supposed to have more education than the woman. Today, there are more women with higher levels of education than before and women with higher levels are less likely to find partners matching this expectation. Being happily single requires being economically self-sufficient and being psychologically independent. Women in this situation may find remarriage much less attractive.
One key factor in understanding some of these issues is the level of continuing parental investment in adult children, and possibly their children. The number of grandparents raising children in the USA is reckoned to be in the vicinity of 2.7 million. In addition, there is the continued support of adult children themselves which can be substantial. The Pew Research document “Helping Adult Children” (2015) gives some indication of the nature and extent of this support, which tends to be even greater in Europe than the USA, with 60% of Italian parents reporting an adult child residing with them most of the year.
Blended Families
Most academic research on reconstituted or blended families focuses on younger adults and the kind of difficulties which ensue when trying to blend children raised by a different spouse/partner and one or more adults with perhaps different views or experience on how this might be accomplished. All sorts of issues can arise: conflicted loyalties, different attitudes to discipline, role-ambiguity, and the simple fact of a far-reaching change easily perceived as a disruption on the part of a child. Given the rise of the gray divorce, it is increasingly the case that this age group will encounter later age, or adult children (sometimes called the “boomerang generation”), in the house of their new partners. Such encounters are even more likely given the rise of the so-called “silver surfer” utilizing online dating sites, and the fact that an increasing number of adult children continue to live at home given the increased cost of housing.
There has not been substantial research on recoupling and blended families in later life, but Papernow (2018) notes that all of the factors normally in play with younger children can be just as present, and even exacerbated, by the fact that previous relationships have had an even longer time to grow and solidify. In addition, stepfamilies formed in later life may have very difficult and complicated decisions to make about estate planning and elder care, as well as navigating daily life together, as an increasing number of young adults live at home (“grown but not gone”).

Papernow lists five challenges for later-life stepfamilies:
- Stepparents are stuck as outsiders, while parents are the insiders in their relationships with their families.
- Stepchildren struggle with the change, even as adults, as they navigate new dynamics in family gatherings, status, and loyalty issues
- Parenting and discipline issues polarize the parents and stepparents. In general, stepparents want more discipline and are viewed as harsher, while parents want more understanding and are viewed more as the pushover. There are often disagreements about how much support (financial, physical, and emotional) to give older children.
- Stepfamilies must build a new family culture, even after there are already at least two established family cultures coming together.
- Ex-spouses are still part of a stepfamily, and children, even adult children, are worse off when they are involved in the conflict between their parents ex-spouses.
Putting It Together: Middle Adulthood
At the beginning of this section we referred to the physical, psychological, and social aspects of middle adulthood. These have ranged from minor physiological changes to the way that knowledge of our own mortality may influence how we behave and feel during this part of the lifespan. The central theme might be identified as that of connection—the way that the body and mind are connected, how one can affect the other, exemplified by the way that physical mobility can impact cerebral acuity. In addition, we have learned that we are more selective in regard to interpersonal connection as we age. The positive aspects of relationships, work, and family assume ever greater importance. Hope is ever present, but these sorts of positive and fulfilling connections cannot be postponed indefinitely. Freud believed that civilization was only possible if humans could be induced, or trained, to defer immediate gratification. That was what the process of primary childhood socialization was about. Perhaps middle adulthood demands that we unlearn this, if only partially. At this stage of the life course, it is now or never. Time is finite and there is none left for indefinite postponement. This is what modern developmental theory has come to understand as mortality salience.
Developmental perspectives have tended to view intimacy and familial relationships as a universal need and function. It has largely left their transformation by divorce, cohabitation and so forth to the sociologists. However, there is now a clearer understanding of the way that structural economic and social change have impacted family structures, often in those least able to resist the disruptive effects of social inequality (Cherlin, 2014). Income and education levels play as large a part in all of this as lifestyle choices, and selectivity. We can only hope that advances in medical science can lead to greater quality of life at this stage of the life course, and that they are made widely available.
References and Resources
Listed below are the references and resources used to curate this module.
Carter, Sarah, et al. (2019). Lifespan Development. Lumen Learning. courses.lumenlearning.com/wm-lifespandevelopment/.
Lally, Martha, and Suzanne Valentine-French (n.d.). FamR 230 – Human Development. LibreTexts Social Sciences. socialsci.libretexts.org/Courses/Hawaii_Community_College_at_Palamanui/FamR_230_-_Human_Development.
Spielman, R.M., et al. (Apr. 2020). Psychology 2e. OpenStax. openstax.org/details/books/psychology-2e.
Taylor, S. E. (2010). Social support: A review. In H. S. Friedman (Ed.), Oxford Handbook of Health Psychology. New York, NY: Oxford University Press.
